
Recommendations for a one-size fits all vaccine will increase diseases in all populations.
Vaccination, probably the most controversial word on the planet!

This site is not about anti-vaccination, neither denying the existence of a virus! Its primary purpose is to inform.
Collecting solid scientific information, subject matter expert articles and interviews. Information mainly neglected by the “main stream media”.
This site is not build to provoke, abuse or deny. Critical definitely, but also open to receive criticism.
“The better the critic, the more holistic the sense of how own perspectives and tastes fit into the diverse pool of informed opinion of others.”
The contact form is available to anyone. If you think information is incorrect please provide documented conclusive material and the the content will be removed.
“Untruth naturally afflicts historical information.
(Muhammad ibn Khaldun al-Hadrami 1379, 1–2Muhammad ibn Khaldun al-Hadrami, Abu Zayd ’Abd ar-Rahman ibn. 1379. Muqaddimat Ibn Khaldun Li-Kitab Al-’ibar Wa-Diwan Al-Mubtada’ Wa-Al-Khabar Fi Ayyam Al-’Arab Wa-Al-’Ajam Wa-Al-Barbar, Wa-Man ’asarahum Min Dhawi Al-Sultan Al-Akbar. Misr : al-Mataba’ah al-Bahiyah al-Misriyah. http://archive.org/details/McGillLibrary-rbsc_isl_kitab-al-ibar_muqaddimah_d167l2361900z-16098.).
There are various reasons that make this unavoidable. One of them is partisanship for opinions and schools. If the soul is impartial in receiving information, it devotes to that information the share of critical investigation the information deserves, and its truth or untruth thus becomes clear.
However, if the soul is infected with partisanship for a particular opinion or sect, it accepts without a moment’s hesitation the information that is agreeable to it. Prejudice and partisanship obscure the critical faculty and preclude critical investigation.
The result is that falsehoods are accepted and transmitted”
I have never been critical against any vaccine whatsoever; have had all my vaccinations in the 60’s, some more serving the Dutch navy (1978) and in 2010 another 3 shots due to business travel.
Rushing a vaccine with a technology never registered anywhere in the world before; for a virus with a global iFR 0.15-0.20% (0.03-0.04% in those <70 years) [source John P. A. Ioannidis] to me is utterly madness.
Anyone with a healthy brain should think beyond general statements broadcasted by the main stream media, be critical, questioning the information and do his/her own research.
‘The WHO recommendations for vaccines are a one-size fits all and this fact means that these policies will increase diseases in all populations.
–Judy Wilyman PhD
They cannot be described as ‘protective health policies’ because they contradict the science of epigenetics; the science showing that individuals are pre-disposed to diseases due to their genetic make-up and the interaction with chemicals in the vaccines.
Translate this blog in Deutsch Italiano Portoghese Española Ελληνικά or any other language
International Covenant on Civil and Political Rights
Adopted and opened for signature, ratification and accession by General Assembly resolution 2200A (XXI) of 16 December 1966
entry into force 23 March 1976, in accordance with Article 49
Article 7
No one shall be subjected to torture or to cruel, inhuman or degrading treatment or punishment. In particular, no one shall be subjected without his free consent to medical or scientific experimentation.
https://www.ohchr.org/EN/ProfessionalInterest/Pages/CCPR.aspx
Council of Europe – Covid-19 vaccines: ethical, legal and practical considerations
Resolution 2361 (2021)
7.1 with respect to the development of Covid-19 vaccines:
7.1.1 ensure high quality trials that are sound and conducted in an ethical manner in accordance with the relevant provisions of the Convention on human rights and biomedicine (ETS No. 164, Oviedo Convention) and its Additional Protocol concerning Biomedical Research (CETS No. 195), and which progressively include children, pregnant women and nursing mothers;
7.1.2 ensure that regulatory bodies in charge of assessing and authorising vaccines against Covid-19 are independent and protected from political pressure;
7.1.3 ensure that relevant minimum standards of safety, efficacy and quality of vaccines are upheld;
7.1.4 implement effective systems for monitoring the vaccines and their safety following their roll-out to the general population, also with a view to monitoring their long-term effects;
7.1.5 put in place independent vaccine compensation programmes to ensure compensation for undue damage and harm resulting from vaccination;
7.1.6 pay special attention to possible insider trading by pharmaceutical executives, or pharmaceutical companies unduly enriching themselves at public expense, by implementing the recommendations contained in Resolution 2071 (2015) on Public health and the interests of the pharmaceutical industry: how to guarantee the primacy of public health interests?
7.1.7 overcome the barriers and restrictions arising from patents and intellectual property rights, in order to ensure the widespread production and distribution of vaccines in all countries and to all citizens;
7.3 with respect to ensuring high vaccine uptake:
7.3.1 ensure that citizens are informed that the vaccination is NOT mandatory and that no one is politically, socially, or otherwise pressured to get themselves vaccinated, if they do not wish to do so themselves;
7.3.2 ensure that no one is discriminated against for not having been vaccinated, due to possible health risks or not wanting to be vaccinated;
https://pace.coe.int/en/files/29004/html
W.H.O Scientists Question Safety Of Vaccines
CAUGHT ON CAMERA: W.H.O Scientists Question Safety Of Vaccines. Shocking footage from inside The W.H.O. Global Vaccine Safety Summit on Dec. 2&3 2019. – 9 minutes
Prof. Heidi Larson, PhD – explains the problems with confidence of health care providers in vaccines
Professor of Anthropology, Risk and Decision Scientist. Director, Vaccine confidence project
… the other thing that’s a trend and an issue is not just confidence in providers but confidence of health care providers.
We have a very wobbly health professional frontline that is starting to question vaccines and the safety of vaccines!
That’s a huge problem because to this day any study I’ve seen and we’re constantly looking on any studies in this space, still the most trusted person on any study I have seen globally is the health care provider and if we lose that we’re in trouble
Global Vaccine Safety Summit Full version
1 hour, 33 minutes
Prof. Heidi Larson PhD – WHO
WHO Global Vaccine Safety Summit about misinformation.
“The problem with misinformation is not so simple, a lot of it is NOT mis-information”
Prof. Heidi Larson PhD
Pandemic Strategies: Lessons and Consequences – International Conference in Stockholm
Jan 21, 2023
Our international conference at the Stockholm Waterfront 21-22 January 2023.
15 leading doctors, researchers and lawyers from the US, Canada, UK, Germany, France, Belgium, Switzerland, Israel, Ukraine and Norway, along with 7 Swedes.
An independent production company was on site to record all angles of the conference and to provide them to the public via this page. Make sure to check back regularly, as we publishing further presentations and interviews over the coming days.
Presentations and panel discussions (3 per day) will be released in the order that they appeared on the program. Interviews and other content to follow shortly…….stay tuned!
https://lakaruppropet.se/international-conference-pandemic-strategies/
Covid19 Vaccination – Listen to the testimony of many medical doctor’s and others.
Maybe most important, Senta Depuydt, a journalist alerting us about the pandemic accelerator act of the European Union (April 2020) allowing vaccine producers to have a free pass for safety.
On July 15 The European Parliament agreed to remove the need of risk evaluation requested under the GMO regulations. That decision was made in 10 days, without scientific reports or hearings in health Commission. No debate and no amendments prior to this vote.
Children’s Health Defense Europe has asked for the annulment of this decision in the European Court of Justice in Luxembourg.
Understand that the current covid vaccines are not proven safe.
Legislators have abandoned the principle of precaution by putting blind faith in a dangerous experiment. The current COVID vaccines are an experimental product based on the injection of genetic material into ourselves and the risk of using these new technologies on humans and the environment are unknown.
They could have Irreversible consequences.
Maybe most important, Senta Depuydt, a journalist alerting us about the pandemic accelerator act of the European Union (April 2020) allowing vaccine producers to have a free pass for safety.
On July 15 The European Parliament agreed to remove the need of risk evaluation requested under the GMO regulations. That decision was made in 10 days, without scientific reports or hearings in health Commission. No debate and no amendments prior to this vote.
Children’s Health Defense Europe has asked for the annulment of this decision in the European Court of Justice in Luxembourg.
Understand that the current covid vaccines are not proven safe.
Legislators have abandoned the principle of precaution by putting blind faith in a dangerous experiment. The current COVID vaccines are an experimental product based on the injection of genetic material into ourselves and the risk of using these new technologies on humans and the environment are unknown.
They could have Irreversible consequences.
Full lenght video:
Sample testimonies:
Dr Andrew Kaufmann This pandemic is not a real medical pandemic.
The COVID-19 vaccine is not proven safe or effective because there is not been enough time. In addition there is not a clear definition of any new disease for which it can be tested against.
There has not been a virus that has been purified or shown to be the cause of an illness thus there is no target for a vaccine.
However the bottom line is that since no additional deaths have a occurred in relation to a new disease there is simply no need for a new vaccine
Dr Vernon Coleman (Minute 3:51)
Doctors aren’t allowed to question COVID-19 in public talking the truth about the alleged
disease and the vaccine.
I’ve been demonised and lied about and a 50 year career and reputation trashed by those promoting a pandemic that never was and a vaccine that was never needed. The whole COVID-19 scam is as I said in March 2020 the greatest hoax in history the principle of informed consent is essential in medicine.
Dr Piotr Rubas internist in Germany. (Minute 17:58)
I strongly disagree to getting vaccinated with this experimental Corona vaccine which is not proven safe or effective.
You should not expose your body to something unknown due to a virus which mortality rate is similar to that of
seasonal influenza virus. This is not a real medical pandemic.
I want you to remember that each one of you every single one of you independently is a beacon of light for those around you. So set the example stand up continue to fight continue to speak out especially for your children let your children see what it means to be free allow your children to witness your heroism and that you are willing to stand up and do what’s right regardless of what’s going on around you
Will covid-19 vaccines save lives? Current trials aren’t designed to tell us
The world has bet the farm on vaccines as the solution to the pandemic, but the trials are not focused on answering the questions many might assume they are. Peter Doshi reports
As phase III trials of covid-19 vaccines reach their target enrolments, officials have been trying to project calm. The US coronavirus czar Anthony Fauci and the Food and Drug Administration leadership have offered public assurances that established procedures will be followed. Only a “safe and effective” vaccine will be approved, they say, and nine vaccine manufacturers issued a rare joint statement pledging not to prematurely seek regulatory review.
But what will it mean exactly when a vaccine is declared “effective”? To the public this seems fairly obvious. “The primary goal of a covid-19 vaccine is to keep people from getting very sick and dying,” a National Public Radio broadcast said bluntly.
Peter Hotez, dean of the National School of Tropical Medicine at Baylor College of Medicine in Houston, said, “Ideally, you want an antiviral vaccine to do two things first, reduce the likelihood you will get severely ill and go to the hospital, and two, prevent infection and therefore interrupt disease transmission.”
Yet the current phase III trials are not actually set up to prove either. None of the trials currently under way are designed to detect a reduction in any serious outcome such as hospital admissions, use of intensive care, or deaths. Nor are the vaccines being studied to determine whether they can interrupt transmission of the virus. https://www.bmj.com/content/371/bmj.m4037
The Safety of COVID-19 Vaccinations
REACT19 – Scientific Publications Directory
Collection of peer reviewed case reports and studies citing adverse effects post COVID vaccination.
Researching Covid vaccine adverse events can be daunting in part due to a broad myriad of factors. Primarily, the information is incredibly challenging to find. Here, we share an ever growing list of peer-reviewed studies specific to Covid vaccine adverse events. This list is curated and maintained by our dedicated staff of injured PhDs and medical professionals.
Before diving in, please take a look at our Research Primer: How to Read and Understand Research for tools to how best approach the massive amount of information found in the document below. As always, this is for informational purposes only. Please discuss with your trusted medical team.
December 22, 2023 – 3,580 entries https://react19.org/science
Round Table Discussion on COVID Vaccines
On Wednesday December 7 2022, Senator Ron Johnson (R-WI) hosted a roundtable discussion
“COVID-19 Vaccines: What They Are, How They Work, and Possible Causes of Injuries” to expose the dangers of the experimental mRNA Covid vaccine.
Peter McCullough, Robert Malone, Ryan Cole, Pierre Kory, Paul Marik, Harvey Risch, Aaron Siri, Esq. (ICAN’s attorney), Edward Dowd, OpenVAERS’ founder, Liz Willner, David Gortler, and others.
COVID-19 mRNA Vaccines: Lessons Learned from the Registrational Trials and Global Vaccination Campaign
Published: January 24, 2024
Mead M, Seneff S, Wolfinger R, et al. (January 24, 2024) COVID-19 mRNA Vaccines: Lessons Learned from the Registrational Trials and Global Vaccination Campaign. Cureus 16(1): e52876. doi:10.7759/cureus.52876
Abstract
Our understanding of COVID-19 vaccinations and their impact on health and mortality has evolved substantially since the first vaccine rollouts. Published reports from the original randomized phase 3 trials concluded that the COVID-19 mRNA vaccines could greatly reduce COVID-19 symptoms. In the interim, problems with the methods, execution, and reporting of these pivotal trials have emerged. Re-analysis of the Pfizer trial data identified statistically significant increases in serious adverse events (SAEs) in the vaccine group. Numerous SAEs were identified following the Emergency Use Authorization (EUA), including death, cancer, cardiac events, and various autoimmune, hematological, reproductive, and neurological disorders. Furthermore, these products never underwent adequate safety and toxicological testing in accordance with previously established scientific standards. Among the other major topics addressed in this narrative review are the published analyses of serious harms to humans, quality control issues and process-related impurities, mechanisms underlying adverse events (AEs), the immunologic basis for vaccine inefficacy, and concerning mortality trends based on the registrational trial data. The risk-benefit imbalance substantiated by the evidence to date contraindicates further booster injections and suggests that, at a minimum, the mRNA injections should be removed from the childhood immunization program until proper safety and toxicological studies are conducted. Federal agency approval of the COVID-19 mRNA vaccines on a blanket-coverage population-wide basis had no support from an honest assessment of all relevant registrational data and commensurate consideration of risks versus benefits. Given the extensive, well-documented SAEs and unacceptably high harm-to-reward ratio, we urge governments to endorse a global moratorium on the modified mRNA products until all relevant questions pertaining to causality, residual DNA, and aberrant protein production are answered.
Conclusions (page 25)
Careful, objective evaluation of COVID-19 mRNA product safety is crucial for upholding ethical standards and evidence-informed decision-making. Our narrative review concerning the registrational trials and the EUA’s aftermath offers evidence-informed insights into how these genetic vaccines were able to enter the market. In the context of the two pivotal trials, safety was never assessed in a manner commensurate with previously established scientific standards either for vaccines or for GTPs, the more accurate classification ofthese products. Many key trial findings were either misreported or omitted entirely from published reports.
The usual safety testing protocols and toxicology requirements were bypassed by the FDA and vaccine manufacturers, and the premature termination of both trials obviated any unbiased assessment of potential SAEs due to an insufficient timeframe for proper trial evaluation. It was only after the EUA that the serious biological consequences of rushing the trials became evident, with numerous cardiovascular, neurological, reproductive, hematological, malignant, and autoimmune SAEs identified and published in the peer reviewedmedical literature.
Moreover, the COVID-19 mRNA vaccines produced via Process 1 and evaluated in the trials were not the same products eventually distributed worldwide; all of the COVID-19 mRNA products released to the public were produced via Process 2 and have been shown to have varying degrees of DNA contamination.
The failure of regulatory authorities to heretofore disclose process-related impurities (e.g., SV40) has further increased concerns regarding safety and quality control oversight of mRNA vaccine manufacturing processes.
Since early 2021, excess deaths, cardiac events, strokes, and other SAEs have often been wrongly ascribed to COVID-19 rather than to the COVID-19 mRNA vaccinations. Misattribution of SAEs to COVID-19 often may be due to the amplification of adverse effects when mRNA injections are followed by SARS-CoV-2 subvariant infection. Injuries from the mRNA products overlap with both PACS and severe acute COVID-19 illness, often obscuring the vaccines’ etiologic contributions. Multiple booster injections appear to cause immune dysfunction, thereby paradoxically contributing to heightened susceptibility to COVID-19 infections with successive doses. For the vast majority of adults under the age of 50, the perceived benefits of the mRNA boosters are profoundly outweighed by their potential disabling and life-threatening harms. Potential harms to older adults appear to be excessive as well. Given the well-documented SAEs and unacceptable harm-torewardratio, we urge governments to endorse and enforce a global moratorium on these modified mRNA products until all relevant questions pertaining to causality, residual DNA, and aberrant protein production are answered.
https://www.cureus.com/articles/203052-covid-19-mrna-vaccines-lessons-learned-from-the-registrational-trials-and-global-vaccination-campaign#!/
References: Page 28-38

Presence of viral spike protein and vaccinal spike protein in the blood serum of patients with long-COVID syndrome
Abstract. – OBJECTIVE: COVID-19 patients experience, in 10-20% of the cases, a prolonged long-COVID syndrome, defined as the persistence of symptoms for at least two months after the infection.
The underlying biological mechanisms of this syndrome remain poorly understood. Several hypotheses have been proposed, among which are the potential autoimmunity resulting from molecular mimicry between viral spike protein and human proteins, the reservoir and viral reproduction hypothesis, and the viral integration hypothesis.
Although official data state that vaccinal spike protein is harmless and remains at the site of infection, several studies proposed spike protein toxicity and found it in blood circulation several months after the vaccination. https://www.europeanreview.org/article/34685
Vaccines Against COVID-19 Worse Than the Disease? Reviewing Some Possible Unintended Consequences of the mRNA
Experimental mRNA vaccines have been heralded as having the potential for great benefits, but they also harbor the possibility of potentially tragic and even catastrophic unforeseen consequences.
The mRNA vaccines against SARS-CoV-2 have been implemented with great fanfare, but there are many aspects of their widespread utilization that merit concern.
We have reviewed some, but not all, of those concerns here, and we want to emphasize that these concerns are potentially serious and might not be evident for years or even transgenerationally.
In order to adequately rule out the adverse potentialities described in this paper, we recommend, at a minimum, that the following research and surveillance practices be adopted:
A national effort to collect detailed data on adverse events associated with the mRNA vaccines with abundant funding allocation, tracked well beyond the first couple of weeks after vaccination.
Repeated autoantibody testing of the vaccine-recipient population. The autoantibodies tested could be standardized and should be based upon previously documented antibodies and autoantibodies potentially elicited by the spike protein. These include autoantibodies against phospholipids, collagen, actin, thyroperoxidase (TPO), myelin basic protein, tissue transglutaminase, and perhaps others.
Immunological profiling related to cytokine balance and related biological effects. Tests should include, at a minimum, IL-6, INF-α, D-dimer, fibrinogen, and C-reactive protein.
Studies comparing populations who were vaccinated with the mRNA vaccines and those who were not to confirm the expected decreased infection rate and milder symptoms of the vaccinated group, whileat the same time comparing the rates of various autoimmune diseases and prion diseases in the same two populations.
Studies to assess whether it is possible for an unvaccinated person to acquire vaccine-specific forms of the spike proteins from a vaccinated person in close proximity.
In vitro studies to assess whether the mRNA nanoparticles can be taken up by sperm and converted into cDNA plasmids.
Animal studies to determine whether vaccination shortly before conception can result in offspring carrying spike-protein-encoding plasmids in their tissues, possibly integrated into their genome.
In vitro studies aimed to better understand the toxicity of the spike protein to the brain, heart, testes, etc. https://ijvtpr.com/index.php/IJVTPR/article/view/23/51
VAERS Analysis Weekly analysis of the VAERS data
I am just a concerned citizen reporting on often overlooked public data regarding adverse events related to the new Covid-19 vaccines. I work with data for a living and have been in the technology field for over two decades.
https://vaersanalysis.info/about/
Official DEATH Signal for Covid-19 jabs was present in VAERS just 1 month after rollout
Quick Summary:
The CDC has been extremely negligent in following its own protocols as far as safety signal analysis for the Covid-19 shots. Their protocols state that they will perform a safety signal analysis on a weekly basis, using something called the Proportional Reporting Ratio (PRR).
As far as anyone knows (and only because of FOIA requests by independent investigators), the CDC had not done the PRR safety signal analysis for the Covid-19 shots prior to March of 2022, which was a full 15 months after the initial rollout. Obviously, you did not hear about any of this, because the CDC didn’t do the safety analysis (or suppressed it).
The CDC VAERS data for death events for the Covid-19 shots triggered a safety signal for DEATH as early as 1/15/2021, just a month or so after the initial rollout. (At that point in time, there were 181 documented deaths in association with the Covid-19 shots.) Obviously, you did not hear about any of this, because the CDC didn’t do the safety analysis (or suppressed it).
If the data is age-stratified, the DEATH safety signal was triggered even earlier; as early as 12/30/2020 for 80+ year olds, and as early as 1/8/2021 for the 60-64, 65-79 year olds. Once again, you did not hear about this, because the CDC didn’t do the safety analysis (or suppressed it).
At a minimum, a further investigation should take place to determine exactly when safety signals were first generated for each of the major symptoms of special interest as identified in their published standard operating procedure (if not for all symptoms).
It is reasonable to conclude that the CDC has been found shockingly derelict in its duty and role to protect public health, and as such it should be obvious that the CDC should be defunded and dismantled immediately and responsible parties brought to justice.
Steve Kirsch’s newsletter
https://stevekirsch.substack.com/
An open letter to CDC director Walensky: Why have you ignored the DEATH safety signal in VAERS for more than 2 years?
I tried billboards to get their answer, but now it’s time to ramp up the campaign. Here’s my email to the CDC director.
Thanks to the brilliant work of VAERS Analysis, we now know that the DEATH safety signal was first triggered in VAERS less than a month after the vaccines rolled out. Nobody at the CDC cared enough to alert the public that a killer vaccine had been unleashed.
Members of Congress are not calling for an investigation. They are doing nothing. Not even a letter to Walensky to ask what’s up.
The mainstream media is doing nothing as usual. No stories. No investigation. The CDC can ignore hundreds of safety signals and that’s just perfectly OK with the media.
So it is clearly my personal responsibility to inform the American people directly that hundreds of safety signals (including death) triggered in VAERS and not only does the CDC know it (we know that from the FOIA requests), but they are doing absolutely nothing to inform the public.
https://stevekirsch.substack.com/p/the-cdc-has-been-ignoring-the-death?utm_source=twitter&utm_campaign=auto_share&r=o7iqo
Pfizer trials more people died in the vaccinated group
In Pfizer’s own trials more people died in the vaccinated group than the placebo group. And now we wonder why highly vaccinated nations have ‘unexplainable’ excess mortality.
SARS-CoV-2 spike mRNA vaccine sequences circulate in blood
First published: 17 January 2023
Full-length or traces of SARS-CoV-2 spike mRNA vaccine sequences were found in blood up to 28 days after COVID-19 vaccination.
https://pubmed.ncbi.nlm.nih.gov/36647776/
Abstract
In Denmark, vaccination against Severe Acute Respiratory Syndrome Corona Virus 2 (SARS-CoV-2) has been with the Pfizer-BioNTech (BTN162b2) or the Moderna (mRNA-1273) mRNA vaccines.
Patients with chronic hepatitis C virus (HCV) infection followed in our clinic received mRNA vaccinations according to the Danish roll-out vaccination plan.
To monitor HCV infection, RNA was extracted from patient plasma and RNA sequencing was performed on the Illumina platform. In 10 of 108 HCV patient samples, full-length or traces of SARS-CoV-2 spike mRNA vaccine sequences were found in blood up to 28 days after COVID-19 vaccination.
Detection of mRNA vaccine sequences in blood after vaccination adds important knowledge regarding this technology and should lead to further research into the design of lipid-nanoparticles and the half-life of these and mRNA vaccines in humans.
https://onlinelibrary.wiley.com/doi/epdf/10.1111/apm.13294
Covid-19 vaccine boosters for young adults: A risk-benefit assessment
‘Unethical’ and up to 98 Times Worse Than the Disease: Top Scientists Publish Paradigm-Shifting Study About COVID-19 Vaccines.
BY JENNIFER MARGULIS AND JOE WANG – SEPTEMBER 10, 202
Study:
Nanotechnology: self assembly structures in mRNA-injections
In this episode of ICIC, Dr Reiner Fuellmich and co-host Dr Mike Yeadon have an insightful conversation with four experts on this explosive topic.
Using dark-field microscopy, Dr David Nixon examines blood samples from people who have been injected with mRNA-based substances and explains the results with corresponding images. Crystalline, unnatural structures are revealed, which change in further observation and show characteristics of a kind of nano- or micro-technology.
Dr. Ana Maria Mihalcea is intensively involved with the ingredients of the Covid mRNA substances. In particular, also with the so-called “shedding effect” of which it is assumed that harmful excretions can be transferred from “vaccinated” to “unvaccinated”.
Karen Kingston, whose research interests include toxicology and the analysis of clinical data as well as the ingredients of the covid mRNA substances, complains that all measures regarding a functioning quality assurance management in the administration of a so-called novel “vaccination” to billions of people worldwide have failed and are still not being implemented after the already poor data situation.
For electrical engineer Shimon Yanowitz, the results of his research have shown that it is a kind of micro-technology, as the injected substances change strangely in the human body and have characteristics of electronic circuits. It is also disturbing that the lipid nanoparticles found in the substances have been approved as “technical devices”, as Karen Kingston reports.
https://video.icic-net.com/w/d45c3f4a-7e9b-4478-be6f-820269343c85
Microscopic Analysis on the Blood After Pfizer/BioNtech or Moderna
The use of dark field microscopic analysis of fresh peripheral blood on a slide was once widespread in medicine, allowing a first and immediate assessment of the state of health of the corpuscular components of the blood.
In the present study we analyzed with a dark field optical microscope the peripheral blood drop from 1006 symptomatic subjects after inoculation with an mRNA injection (Pfizer/BioNTech or Moderna), starting from March 2021.
There were 948 subjects (94% of the total sample ) whose blood showed aggregation of erythrocytes and the presence of particles of various shapes and sizes of unclear origin one month after the mRNA inoculation.
In 12 subjects blood was examined with the same method before vaccination, showing a perfectly normal hematological distribution.
The alterations found after the inoculation of the mRNA injections further reinforce the suspicion that the modifications were due to the so called “ vaccines themselves.
We report 4 clinical cases, chosen as representative of the entire case series. Further studies are needed to define the exact nature of the particles found in the blood and to identify possible solutions to the problems they are evidently causing.
Of the 1006 cases analyzed, only 58 (27 males and 31 females), equal to 5.77% of the total, presented a completely normal hematological picture upon microscopic analysis after the last mRNA injection with either the Moderna or Pfizer concoction. The vaccines are purported to contain at least the spike protein from SARS-CoV-2 (Nance &Meier, 2021), but is known also to contain foreign particles that the CDC and the many promoters of the experimental injections claimed were not in them at all. Among those foreign components are metallic objects as demonstrated previously in this journal by Lee et al. (2022) which are confirmed in our results as described in the following.
The 4 clinical cases reported below, with photographic documentation revealing strange phenomena in their blood, illustrate the range and types of the anomalies found in the microscopic examination of the blood of 94.23% of the 1006 cases (a total of 948 cases that showed the same sorts of abnormalities).
The 4 cases summarized and illustrated here are, according to our understanding and in our opinion as clinical experts,absolutely representative of all 948.
Public Health and Medical Professionals for Transparency
This nonprofit, made up of public health professionals, medical professionals, scientists, and journalists exists solely to obtain and disseminate the data relied upon by the FDA to license COVID-19 vaccines. The organization takes no position on the data other than that it should be made publicly available to allow independent experts to conduct their own review and analyses. Any data received will be made public on this website.
Four days after the Pfizer vaccine was approved for ages 16+, we submitted a Freedom of Information Act Request to the FDA for all of the data within Pfizer’s COVID-19 vaccine biological product file. We have now sued the FDA for not releasing the data.
Follow this link for court documents and for productions of Pfizer’s documents from the FDA.
Covid-19 vaccines and treatments: we must have raw data, now
January 19, 2022 Data should be fully and immediately available for public scrutiny.
In the pages of The BMJ a decade ago, in the middle of a different pandemic, it came to light that governments around the world had spent billions stockpiling antivirals for influenza that had not been shown to reduce the risk of complications, hospital admissions, or death. The majority of trials that underpinned regulatory approval and government stockpiling of oseltamivir (Tamiflu) were sponsored by the manufacturer; most were unpublished, those that were published were ghostwritten by writers paid by the manufacturer, the people listed as principal authors lacked access to the raw data, and academics who requested access to the data for independent analysis were denied.1 2 3 4
Unacceptable delay
Pfizer’s pivotal covid vaccine trial was funded by the company and designed, run, analysed, and authored by Pfizer employees. The company and the contract research organisations that carried out the trial hold all the data.17 And Pfizer has indicated that it will not begin entertaining requests for trial data until May 2025, 24 months after the primary study completion date, which is listed on ClinicalTrials.gov as 15 May 2023 (NCT04368728).
Among regulators, the US Food and Drug Administration is believed to receive the most raw data but does not proactively release them. After a freedom of information request to the agency for Pfizer’s vaccine data, the FDA offered to release 500 pages a month, a process that would take decades to complete, arguing in court that publicly releasing data was slow owing to the need to first redact sensitive information. 2 3 This month, however, a judge rejected the FDA’s offer and ordered the data be released at a rate of 55 000 pages a month. The data are to be made available on the requesting organisation’s website (phmpt.org). https://www.bmj.com/content/376/bmj.o102
Public Health and Medical Professionals for Transparency
This nonprofit, made up of public health professionals, medical professionals, scientists, and journalists exists solely to obtain and disseminate the data relied upon by the FDA to license COVID-19 vaccines. The organization takes no position on the data other than that it should be made publicly available to allow independent experts to conduct their own review and analyses. Any data received will be made public on this website.
Four days after the Pfizer vaccine was approved for ages 16+, we submitted a Freedom of Information Act Request to the FDA for all of the data within Pfizer’s COVID-19 vaccine biological product file. We have now sued the FDA for not releasing the data. Click below for court documents and for productions of Pfizer’s documents from the FDA.
We Should Rethink the Policy
The NNTV (the number needed to vaccinate) is between 200–700 to prevent one case of COVID-19 for the mRNA vaccine marketed by Pfizer, while the NNTV to prevent one death is between 9000 and 50,000 (95% confidence interval), with 16,000 as a point estimate.
The number of cases experiencing adverse reactions has been reported to be 700 per 100,000 vaccinations.
Currently, we see 16 serious side effects per 100,000 vaccinations, and the number of fatal side effects is at 4.11/100,000 vaccinations. For three deaths prevented by vaccination we have to accept two inflicted by vaccination.
Conclusions: This lack of clear benefit should cause governments to rethink their vaccination policy.
https://www.mdpi.com/2076-393X/9/7/693/htm
Why should current Covid-19 vaccines not be used for mass vaccination during a pandemic?
Dr G. Vanden Bossche, DVM, PhD -Independent Vaccine Research Consultant
Dear colleagues at the WHO, my name is Geert Vanden Bossche (GvdB).
My background is veterinary medicine. I’m a certified expert in microbiology and infectious diseases. I have a PhD in Virology and I have a long-standing career in human vaccinology.
I’m urging you to immediately open the scientific debate on how human interventions in the COVID-19 pandemic are currently driving viral immune escape.
I’m urging you to invite me for a scientific hearing open to the public and to scientists all over the world on this very topic. Ignoring or denying the impact of stringent infection prevention measures combined with mass vaccination using prophylactic vaccines is a colossal blunder.
Please do listen to my cry of distress and let’s first and foremost deliberate, on a scientifically justified strategy. To mitigate the tsunami of morbidity and lethality that is now threatening us.
And let’s meanwhile derive a strategy to eradicate the steadily emerging highly infectious variants. On behalf of humanity, I sincerely thank you for considering my call.
Dr G. Vanden Bossche, DVM, PhD -Independent Vaccine Research Consultant
Vaccines Summit Ohio 2021, March 1-3, 2021, Ohio, USA Presentation Dr G. Vanden Bossche
GvdB Sharing his perspective on mass vaccination in COVID-19
Geert Vanden Bossche PhD, an internationally recognised vaccine developer having worked as the head of the Vaccine Development Office at the German Centre for Infection Research.
Coordinated Global Alliance for Vaccines and Immunisation’s Ebola Vaccine Program and contributed to the implementation of an integrated vaccine work plan in collaboration with Global Health Partners (WHO, Bill & Melinda Gates Foundation, CDC, UNICEF), regulators (FDA) and vaccine manufacturers to enable timely deployment or stockpiling of Ebola vaccine candidates.
Highlighting the principle of using a prophylactic vaccine in the midst of a pandemic. Likely to create more more viral variants in the process. Sharing his perspective on mass vaccination in COVID-19.
Deep Dive Questions and Answers with GvdB and Dr Philip McMillan
Dr Vernon Coleman – March 13, 2021
Now more than ever, I need your help. Unless we work together, we are doomed.
I need your help because we need to reach millions with this video and with the big platforms and the mainstream media having banned me, I can’t reach those millions without you. I believe this is the most important video. I will ever make and the most important you will ever see.
I fear that the genocidal lunatics, the horsemen of the Apocalypse who planned this fraud are leading us into Armageddon.
Millions have received one of the COVID-19 vaccines may die as a result of those vaccinations. But the politicians and the advisers did everything wrong. And those who questioned what was happening were demonised and silenced.
The public were originally assured that only through a huge vaccination program could they possibly win back some of their last freedoms. This was always dangerous nonsense.
The 1st problem is that these experimental vaccines have already proved to be desperately dangerous, killing many people already and producing serious adverse events in many more. The size of this particular problem can be judged by the fact that even the authorities admit that probably only one in 100 vaccine related deaths and serious injuries will be reported. It’s impossible to estimate how many will die of allergy problems, heart trouble, strokes, neurological problems, and so on. Or how many would be blinded or paralysed?
The 2nd problem is the immune system problem, known as pathogenic priming or cytokine storm. What happens is that the immune system of the person who’s been vaccinated will be primed to respond in a very dramatic way If that individual comes into contact with the virus in the future.
The result can be catastrophic, and this is what I fear will happen in the autumn and during next winter. The people who’ve had the vaccine are going to be in real trouble when they next come into contact with the coronavirus. Their immune systems will overreact, and that’s likely to be when they will be lots of deaths.
Patients haven’t been officially warned about this problem, although the evidence was published in the International Journal of Clinical Practice for October last year. The paper entitled Informed Consent Disclosure to vaccine trial subjects of risk of COVID-19 vaccines worsening clinical disease. But there’s been no informed consent for patients, and I suspect that most doctors remain ignorant of the risks.
Patients are being told that there are no dangers with these vaccines. The elderly and those with poor immune systems are particularly likely to be killed.
The coronavirus spreads most rapidly in autumn and winter. As a result of the epidemic of illnesses and deaths that will take place, governments will start promoting the next round of vaccinations. There will be much talk of mutations and new horridly prepared experimental vaccines will be produced and heavily promoted.
And this brings us to the 3rd problem, a problem. I don’t think they expected. This problem is just being outlined by Dr Geert Vanden Bossche, who’s a very eminent vaccine specialist. Indeed, I was originally skeptical about what he said because Dr Vanden Bossche has previously worked with Gavin, the Gates Foundation. He’s the last person in the world who could be described as being opposed to vaccination. He pointed out that the vaccines which are currently being used are the wrong weapons to use for this war against the virus infection. Disastrously by giving vaccines to millions, teaching the virus, how to mutate and to become stronger and more deadly.
Trying to devise new vaccines for new mutations simply makes things worse because the scientists can’t possibly get ahead of the mutated viruses and the people who have been vaccinated and now sharing mutated viruses with those around them from the mutations are becoming stronger and deadlier. Ending the lockdowns will be perfectly timed to ensure that new mutations of the COVID-19 virus are spread far and wide.
There’s another associated problem too. Normally our bodies contain white blood cells, which help us defeat infections cells called NK cells. Once the NK cells have done their work our antibodies appear and clean up the mess.
However, Dr Vanden Bossche explains that the COVID-19 vaccines are triggering the production of very specific antibodies which compete with the natural defences of the individuals who’ve had the vaccines.
The Natural defence systems of those who been vaccinated are being suppressed because the specific antibodies which have been produced by the vaccine just take over, and these specific antibodies, the ones produced by the vaccines, are permanent there forever within the bodies of the people who had been vaccinated.
The disastrous result is that the natural immune systems of the 10s or hundreds of millions who are having the vaccines are being effectively destroyed.
Their immune systems will not be able to fight any mutated variation of the virus which develops within their bodies.
And those mutated viruses can spread out into the community. I believe This is why new virus variations are appearing in areas where the vaccine has been given to lots of people.
The bottom line is that giving the vaccines will give the virus an opportunity to become infinitely more dangerous. Every vaccinated individual has the potential to become a mass murderer because their bodies are becoming laboratories, making lethal viruses and worse still, some of the vaccinated individuals may become asymptomatic carriers, spreading lethal viruses around them.
The people who’ve had the vaccine won’t be able to respond to the mutations because their immune systems have been taken over by an artificial defence system given to them by the vaccine. Undesigned to combat the original form of the COVID-19 virus. The vaccinated individuals are going to be very much at risk when the new mutations start to spread.
Giving new vaccines won’t help because the mutated virus will not be vulnerable. The scientists who are making vaccines won’t be able to get ahead of the mutating virus.
If Dr Vanden Bossche is right and I believe he is, then it’s the vaccinated individuals who are going to threaten mankind. They’ll be a major threat to anyone who’s been vaccinated. But they’ll also be a major threat to the under vaccinated because the viruses there shedding are going to be more dangerous than the original one.
We are in very dangerous territory if we don’t stop this vaccine program now, then it’s no exaggeration to say that the very future of mankind is at risk.
Evidence for increased breakthrough rates of SARS-CoV-2 variants of concern in BNT162b2-mRNA-vaccinated individuals
Apprehension exists that variants of concern (VOCs) may evade vaccine protection, due to evidence of reduced neutralization of the VOCs B.1.1.7 and B.1.351 by vaccine sera in laboratory assays.
https://www.nature.com/articles/s41591-021-01413-7
SARS-CoV-2 immunity-escape variants, 7 January 2021
Paper prepared by academics for NERVTAG on viral evasion during antibody treatment of the new SARS-CoV 2 immunity-escape variants. It was considered at SAGE 75 on 7 January 2021.
- Concerns have been raised about the possible emergence of SARS-CoV-2 variants that escape immune recognition because of:
- The recent identification of two SARS-CoV-2 variants (one in the UK and the other in South Africa) with apparently increased transmission and substitutions in the receptor binding domain (RBD) on the spike protein that theoretically might be associated with immune escape;
- High levels of SARS-CoV-2 incidence in the community in the UK associated with a variant B.1.1.7;
- The decision in the UK to provide the second dose of SARS-CoV-2 vaccine at 12 weeks rather than 3 weeks after the first dose.
- This paper explores the possibility that SARS-CoV-2 escape variants that are partially or fully resistant to natural immunity, vaccination or antibody therapies may have arisen or will arise.
Particularly in immune suppressed individuals with prolonged viral replication, viral evasion can occur during antibody-based treatment. However, the overall impact of these escape variants on clinical and virological outcomes are not clear.
https://www.gov.uk/government/publications/sars-cov-2-immunity-escape-variants-7-january-2021
Circulating SARS-CoV-2 variants escape neutralization by vaccine-induced humoral immunity
ongoing surveillance has revealed the emergence of variants harboring mutations in spike, the main target of neutralizing antibodies.
Cross-neutralization of B.1.351 variants was weak and comparable to SARS-CoV and bat-derived WIV1-CoV, suggesting that a relatively small number of mutations can mediate potent escape from vaccine responses.
While the clinical impact of neutralization resistance remains uncertain, these results highlight the potential for variants to escape from neutralizing humoral immunity and emphasize the need to develop broadly protective interventions against the evolving pandemic.
In summary, our data highlights the challenges facing all vaccines whose designs were finalized early in the pandemic and based on the sequence of the first-reported virus from Wuhan, China.
https://www.medrxiv.org/content/10.1101/2021.02.14.21251704v1.full
Multiple SARS-CoV-2 variants escape neutralization by vaccine-induced humoral immunity
Highlights
• Numerous variants of SARS-CoV-2-harboring mutations in spike have arisen globally
• mRNA vaccines elicit potent neutralizing activity against homologous pseudovirus
• Cross-neutralization of strains with receptor-binding domain (RBD) mutations is poor
• Both RBD and non-RBD mutations mediate escape from vaccine-induced humoral immunity
Summary
Vaccination elicits immune responses capable of potently neutralizing SARS-CoV-2. However, ongoing surveillance has revealed the emergence of variants harboring mutations in spike, the main target of neutralizing antibodies. To understand the impact of these variants, we evaluated the neutralization potency of 99 individuals that received one or two doses of either BNT162b2 or mRNA-1273 vaccines against pseudoviruses representing 10 globally circulating strains of SARS-CoV-2. Five of the 10 pseudoviruses, harboring receptor-binding domain mutations, including K417N/T, E484K, and N501Y, were highly resistant to neutralization. Cross-neutralization of B.1.351 variants was comparable to SARS-CoV and bat-derived WIV1-CoV, suggesting that a relatively small number of mutations can mediate potent escape from vaccine responses. While the clinical impact of neutralization resistance remains uncertain, these results highlight the potential for variants to escape from neutralizing humoral immunity and emphasize the need to develop broadly protective interventions against the evolving pandemic.
https://www.cell.com/cell/fulltext/S0092-8674(21)00298-1
SARS-CoV-2 variants B.1.351 and P.1 escape from neutralizing antibodies
Highlights
• B.1.1.7, B.1.351 and P.1 do not show augmented host cell entry
• Entry inhibitors under clinical evaluation block all variants
• B.1.351 and P.1 can escape from therapeutic antibodies
• B.1.351 and P.1 evade antibodies induced by infection and vaccination
Summary
The global spread of SARS-CoV-2/COVID-19 is devastating health systems and economies worldwide. Recombinant or vaccine-induced neutralizing antibodies are used to combat the COVID-19 pandemic. However, the recently emerged SARS-CoV-2 variants B.1.1.7 (UK), B.1.351 (South Africa) and P.1 (Brazil) harbor mutations in the viral spike (S) protein that may alter virus-host cell interactions and confer resistance to inhibitors and antibodies. Here, using pseudoparticles, we show that entry of all variants into human cells is susceptible to blockade by the entry inhibitors soluble ACE2, Camostat, EK-1 and EK-1-C4. In contrast, entry of the B.1.351 and P.1 variant was partially (Casirivimab) or fully (Bamlanivimab) resistant to antibodies used for COVID-19 treatment. Moreover, entry of these variants was less efficiently inhibited by plasma from convalescent COVID-19 patients and sera from BNT162b2 vaccinated individuals. These results suggest that SARS-CoV-2 may escape neutralizing antibody responses, which has important implications for efforts to contain the pandemic.
https://www.cell.com/cell/fulltext/S0092-8674(21)00367-6
mRNA Vaccine Induced Damage mechanisms
Dr. Loretta Bolgan
The various mechanisms by which COVID-19 vcaccines can induce immunopathologies.
Sars-Cov-2, could certinaly be responsible for the phenomenon of disease enhancement in vaccinees, which should have been investigated and excluded before proceeding with human trials.
Given the similarity between the mechanisms of COVID-19 damage and vaccine adverse reactions, it is conceivable that many of the symptoms and pathologies associated with long-COVID may also be present as long-term consequences of vaccination.
Long read -34 pages: Original italian language English version
INFORMED CONSENT
Informed consent disclosure to vaccine trial subjects of risk of COVID-19 vaccines worsening clinical disease
Results of the study: COVID-19 vaccines designed to elicit neutralising antibodies may sensitise vaccine recipients to more severe disease than if they were not vaccinated. Vaccines for SARS, MERS and RSV have never been approved, and the data generated in the development and testing of these vaccines suggest a serious mechanistic
concern:
that vaccines designed empirically using the traditional approach (consisting of the unmodified or minimally modified coronavirus viral spike to elicit neutralising antibodies), be they composed of protein, viral vector, DNA or RNA and irrespective of delivery method, may worsen COVID-19 disease via antibody-dependent enhancement (ADE).
This risk is sufficiently obscured in clinical trial protocols and consent forms for ongoing COVID-19 vaccine trials that adequate patient comprehension of this risk is unlikely to occur, obviating truly informed consent by subjects in these trials.
CONCLUSION
Given the strong evidence that ADE is a non-theoretical and compelling risk for COVID-19 vaccines and the “laundry list” nature of informed consents, disclosure of the specific risk of worsened COVID-19 disease from vaccination calls for a specific, separate, informed
consent form and demonstration of patient comprehension in order to meet medical ethics standards.
The informed consent process for ongoing COVID-19 vaccine trials does not appear to meet this standard.
While the COVID-19 global health emergency justifies accelerated vaccine trials of candidates with known liabilities, such an acceleration is not inconsistent with additional attention paid to heightened informed consent procedures specific to COVID-19 vaccine risks.
https://pubmed.ncbi.nlm.nih.gov/33113270/
https://onlinelibrary.wiley.com/doi/epdf/10.1111/ijcp.13795
COVID-19 VACCINE INGREDIENTS
Published August 31, 2021 – Updated October 1, 2021
On 20 August 2021 Dr. Robert Young published his team’s findings after analysing the four dominant COVID-19 “vaccines” using Phase Contrast Microscopy, Transmission and Scanning Electron Microscopyand Energy-Dispersive X-ray Spectroscopy. Their research both confirms and expands upon the priorinvestigations carried out by Dr. Pablo Campra (University of Almeria, Spain), Dr. Juan F. Gastón Añaños(Hospital de Barbastro, Spain), as well as the recent pathology reports from autopsies of vaccinated deceased which were carried out by Prof. Dr. Arne Burkhardt, Prof. Dr. Walter Lang and Prof. Dr. Peter Schirmacher (Germany & Austria).
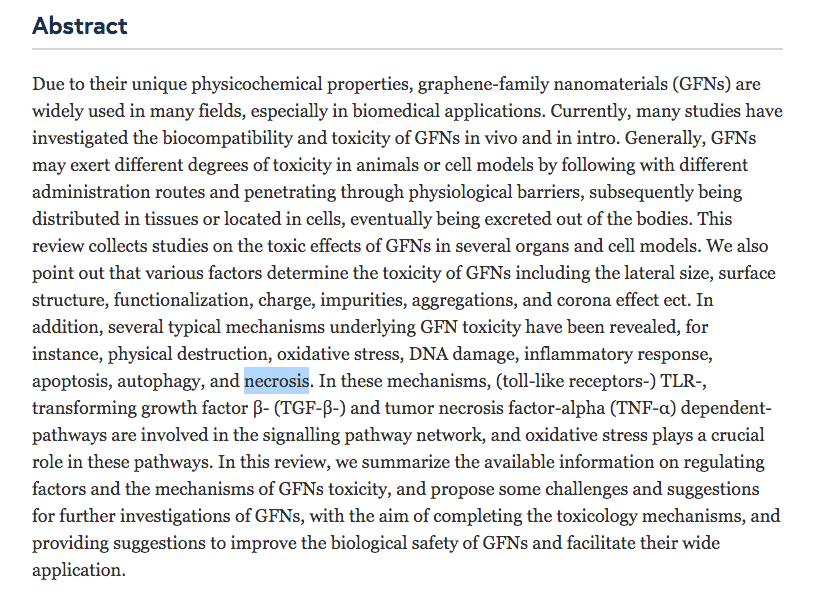
Many of these substances were observed as being bonded to graphene oxide and metallic nanoparticles. GO nanoparticles are necrotic, able to pass into or through physiological barriers including (but not limited to) the blood-air barrier, the blood-testis barrier, the blood-brain barrier, and the blood-placenta barrier. Over a period of several months after intramuscular injection, as much as 75% of the GO nanoparticle “delivery platform”, and most of the substances listed below, are transported extensively throughout the bodies of mammals, into the blood, brain and other organs. Some of the many toxic effects of graphene oxide are myocarditis and blood clotting. Contamination in vaccines appears to be so common that one might be forgiven for thinking that it is deliberate.
https://nobulart.com/covid-19-vaccine-ingredients/
{kind=link}
Scientists vaccine opinions
mRNA: Vaccine or Gene Therapy? The Safety Regulatory Issues
International Journal of Molecular Sciences
Int. J. Mol. Sci. 2023, 24, 10514. https://doi.org/10.3390/ijms241310514
Abstract: COVID-19 vaccines were developed and approved rapidly in response to the urgency created by the pandemic. No specific regulations existed at the time they were marketed.
The regulatory agencies therefore adapted them as a matter of urgency. Now that the pandemic emergency has passed, it is time to consider the safety issues associated with this rapid approval. The mode of action of COVID-19 mRNA vaccines should classify them as gene therapy products (GTPs), but they have been excluded by regulatory agencies.
Some of the tests they have undergone as vaccines have produced non-compliant results in terms of purity, quality and batch homogeneity.
The wide and persistent biodistribution of mRNAs and their protein products, incompletely studied due to their classification as vaccines, raises safety issues.
Post-marketing studies have shown that mRNA passes into breast milk and could have adverse effects on breast-fed babies. Long-term expression,
integration into the genome, transmission to the germline, passage into sperm, embryo/fetal and perinatal toxicity, genotoxicity and tumorigenicity should be studied in light of the adverse events reported in pharmacovigilance databases.
The potential horizontal transmission (i.e., shedding) should also have been assessed. In-depth vaccinovigilance should be carried out. We would expect these controls to be required for future mRNA vaccines developed outside the context of a pandemic.
Professor Christine Stabell Benn
http://www.edctp.org/about-us/scientific-advisory-committee/professor-benn/

https://unherd.com/thepost/study-into-mrna/
Interview minute 9-12
We were so curious to find out when we heard about these two new vaccine types, to find out whether they would behave as live or non live vaccines, because we really didn’t have a clue.
They’re both both the mRNA vaccines and the adenovirus vector vaccines both new vaccine types and and we haven’t got any experience with their potential nonspecific effects.
So we haven’t got an idea whether there were nonspecific effects, whether they were beneficial or potentially harmful.
What we knew and pointed out right from the beginning was that it is a flaw in our system for testing vaccines. We don’t assess the effect of vaccines on all cause mortality, all cause morbidity. We don’t actually get a chance to assess whether they have nonspecific effects.
And it is beyond doubt now that vaccines have nonspecific effects. So it is really a a major flaw in the system.
What we are really worried about was the fact that the whole evaluation of the vaccines focused on the COVID specific effects.
Did the vaccine protects against it, protect against COVID but and and also that the clinical trials were abrogated all after two to four months when the vaccines got emergency approval.
So that means that we only had a very short term to follow up. To actually assess the the full effect of the vaccines both against COVID ….
But for the non specific effects this was a particular problem because nonspecific effects continue to occur months after you have received your vaccine and and we really didn’t have a chance because the randomized clinical trials, the phase three trials were abrogated with the vaccination of the control groups we didn’t have a chance to assess long term effects.
Robert Malone, Theo Schetters – mRna vaccins and the rise of the all-cause mortality rate.
August 2022 – This conversation with Theo Schetters and Robert Malone at “de nieuwe wereld” has been taken down by YouTube. They may not post anything for one week.
https://denieuwewereld.tv/ a platform that brings together people from different disciplines to reflect on major changes that are coming due to a combination of rapid technological developments and globalization.
It is an initiative of philosopher Ad Verbrugge in collaboration with Marlies Dekkers, Jelle van Baardewijk and Willem de Witte.
Widespread Vaccine Failure is the Reproducibility Crisis in Public Health
Will They Adopt Science or Continue a Failing Denialist Agenda?
James Lyons-Weiler Feb 18, 2022
In my podcast, “Unbreaking Science”, my initial goal was to bring guests on who were willing to discuss the perils of continuing down a path on which data manipulation and other less egregious problems with observational studies as conducted in public health. The goal was not iconoclastic; rather, it was to help nudge Science into a position in which critical analysis of individual studies – and sets of studies if need be – was again considered normal and healthy – even if the consequence of that analysis was to draw vaccine safety into question.
The goal of science – understanding and discovery – are at complete odds with taboo against rational criticism of vaccines. Rational criticism is usually conducted via peer-review; however, CDC’s main publication outlet, Morbidity and Mortality Weekly Report, is not peer-reviewed.
What has happened in the public health literature is an inversion of rational thought. Studies (like mine) that identify potential problems with vaccines are targeted for retraction. If Science is a way of knowing, then the quest of scientists should be the truth, that is, reality. The quest to have our knowledge match reality as closely as possible is not possible when the goal of those who claim they are conducting science is to prevent rational criticism at all costs – as if the vaccine science literature is thorough, complete, and finished, at least on the question of benefits and risks – and also as if each and every vaccine recommended by ACIP is the same entity year after year.
https://popularrationalism.substack.com/p/widespread-vaccine-failure-is-the
Peter McCullough, MD, MPH speaks at the 78th Annual Meeting of AAPS on October 2, 2021.
Winning the War Against Therapeutic Nihilism & Trusted Treatments vs Untested Novel Therapies
Dr Robert Malone The truth about the COVID mRNA Vaccines
https://www.rwmalonemd.com/about-us
Dr. Malone is the discoverer of in-vitro and in-vivo RNA transfection and the inventor of mRNA vaccines, while he was at the Salk Institute in 1988. His research was continued at Vical in 1989, where the first in-vivo mammalian experiments were designed by him. The mRNA, constructs, reagents were developed at the Salk institute and Vical by Dr. Malone. The initial patent disclosures were written by Dr. Malone in 1988-1989. Dr. Malone was also an inventor of DNA vaccines in 1988 and 1989. This work results in over 10 patents and numerous publications, yielding about 7000 citations for this work. Dr. Malone was also an inventor of DNA vaccines in 1988 and 1989.
Dr. Byram Bridle, University of Guelph
Alex talks with Dr. Byram Bridle, an Associate Professor on Viral Immunology at the University of Guelph about a new peer-reviewed study that suggests there may be terrifying reasons side effects such as heart inflammation, VITT, and other serious issues may occur in those who have been vaccinated.
Alex: you’ve been very, you know, very open on this whole issue, and you’re not anti vaccine by any stretch. But what do you think about this? Inflammation in the heart and is it an actual threat?”
Dr Bridle: I’m very much pro vaccine, but always making sure that the science is done properly and that we follow the science carefully before going into public rollout of vaccines. – I’ll forewarn you and your listeners that the story I’m about to tell is a bit of a scary one.
The corona virus has a spike protein on its surface. That spike protein allows to infect our bodies. That is why we’ve been using the spike protein in our vaccines. The vaccines we’re using get the cells in our body to manufacture that protein.
If we can mount immune response against that protein, in theory we can prevent this virus from infecting the body. That’s the theory behind the vaccine, however, when studying the disease severe COVID-19, everything that you described earlier, heart problems, lots of problems with cardiovascular system, bleeding and clotting is also related with severe COVID-19.
What has been discovered by scientific community is the spike protein on its own is almost entirely responsible for the damage the cardiovascular system.
If you inject the purified spike protein into the blood of research animals, they get all kinds of damage the cardiovascular system, it can cross the blood brain barrier and cause damage to the brain. Now at first glance, that doesn’t seem too concerning because we’re injecting these vaccines into the shoulder muscle. The assumption until now has been that these vaccines behave like all of our traditional vaccines; that they don’t go anywhere, they stay in our shoulder. Some of the protein will go to the local draining lymph node in order to activate the immune system.
However, this is where the cutting edge science has come in, and this is where it gets scary. Through a request for information from the Japanese Regulatory agency, myself and several international collaborators we have been able to get access to what’s called the Bio-distribution study. It’s the first time ever that scientists have been privy to seeing where these messenger RNA vaccines go after vaccination.
Is it a safe assumption that it stays in the shoulder muscle? The short answer is absolutely not, It’s very disconcerting.
The spike protein gets into the blood, circulates through the blood post-vaccination for several days, it accumulates in the blood, and accumulates in a number of tissues, such as the spleen, bone marrow, the liver, the adrenal gland and of particular concern for me is it accumulates in the ovaries, in quite high concentrations.
Another scientific paper just accepted for publication about 13 young health care workers that received the Moderna vaccine, confirmed that they found the spike protein in circulation in 11 of them.
What this means is: we have known for a long time that the spike protein is a pathogenic protein. It is a toxin that can cause damage in our body if it gets into circulation. Now we have clear cut evidence that when in circulation, the spike protein can do one of two things that can either cause platelets to clump that can lead to clotting. That’s exactly why we’ve been seeing clotting disorders associated with these vaccines. That’s why we’re seeing heart problems. The protein can also cross the blood brain barrier and cause neurological damage.
The following has not yet been accepted for publication:
They were trying to show that the antibodies from the vaccine get transferred through breast milk and the idea was this may be a good thing, ’cause it would confer some passive protection to babies. However, what they found inadvertently was that the vaccines actually get transferred through the birth breast milk; the vaccine vector itself. Any proteins in the blood will get concentrated in breast milk. Looking into the adverse event database in the United States, we have found evidence of suckling infants experiencing bleeding disorders in the gastrointestinal tract. This has implications for blood donation right now. We don’t want transfer of these pathogenic spike proteins to fragile patients being transfused with that blood.
We thought the spike protein was a great target antigen, we never knew the spike protein itself was a toxin. By vaccinating people we are inadvertently inoculating them with a toxin.
I have many other legitimate questions about the long term safety.
Circulating SARS-CoV-2 Vaccine Antigen Detected in the Plasma of mRNA-1273 Vaccine Recipients
Abstract
SARS-CoV-2 proteins were measured in longitudinal plasma samples collected from 13 participants who received two doses of mRNA-1273 vaccine. 11 of 13 participants showed detectable levels of SARS-CoV-2 protein as early as day one after first vaccine injection. Clearance of detectable SARS-CoV-2 protein correlated with production of IgG and IgA.
https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciab465/6279075
Lipid nanoparticles are designed to be widespread throughout the body.
These vaccines and or the spike proteins can cross the blood brain barrier and get into the Brain. Adverse events related to the vaccine seemed to be similar to severe COVID-19; damage to the heart, damage to blood vessels, clotting, bleeding, and neurological issues.
People have to understand the history behind these lipid nanoparticles, these little bubbles of fat we put these messenger RNA’s into. People don’t realize these were never designed for vaccine use. They were designed for gene therapy, not for vaccine use.
They were designed to serve gene therapy and for drug delivery systems. They actually wanted widespread distribution; designed to be widespread throughout the body.
Fast COVID-19 vaccine timelines are unrealistic and put the integrity of scientists at risk
June 17, 2020 Byram W. Bridle, University of Guelph and Shayan Sharif, University of Guelph
We are academic scientists who manage vaccine research programs. In fact, Dr. Bridle received COVID-19-focused funding to develop a novel vaccine platform. Although many of us are working hard towards developing vaccines against SARS-CoV-2, we worry that some in the scientific community have offered too much hope for this to be accomplished in a timely fashion. Sometimes these promises are used by politicians and governments to inform public policies. As a result, the integrity of the scientific community is now in the limelight and, arguably, at risk.
Lessons from SARS and MERS
Educators often rely on past performance to predict the future performance of students. In this respect, how was the performance of the scientific community in the wake of the original SARS-CoV, or Middle East respiratory syndrome (MERS)-CoV? The fact is, no vaccine against a coronavirus has successfully navigated the rigours of clinical testing, despite having up to 17 years to do so.
The same applies to other dangerous respiratory pathogens, such as respiratory syncytial virus. Whether enough has been learned from these past experiences to get the design of COVID-19 vaccines right remains to be seen, and still does not negate the need for a rigorous testing process that will take time.
One concern is that some vaccines can protect against disease (that is, the outcome of an infection) but not against infection (the ability of the virus to get into the body). In this scenario, vaccinated individuals could potentially become asymptomatic carriers of SARS-CoV-2, thereby spreading COVID-19. For this and many other reasons, a cautious approach must be taken to developing COVID-19 vaccines.
https://ovc.uoguelph.ca/news/fast-covid-19-vaccine-timelines-are-unrealistic-and-put-integrity-scientists-risk (This article is republished from The Conversation under a Creative Commons license. Read the original article.)
Dr Byram Bridle – I would probably prefer to have natural immunity
I’m a viral immunologist. That means I have expertise in the fields of virology and immunology.
I do have a COVID-19 vaccine development program going on. And the vaccines that we’re developing realistically wouldn’t be able to go into human clinical trials for at least another year and a half, maybe two years.
But I want to highlight that vaccine hesitancy is very, very different. And a lot of people who have the vaccine hesitancy are being made to feel very bad these days, right? It’s as though if they were simply educated enough about vaccines, then they would have no problem with these COVID-19 vaccines. But that’s not the case. That’s not the definition, certainly that I use. These are individuals instead who are unsure of their commitment to taking a vaccine. And it’s usually because of outstanding questions. So in other words, the onus is not on the individual. It’s not that the individual simply needs to be educated. We have, there’s lots of people who are very deep thinkers about this, doing their own research about the COVID-19 vaccines and coming up with very legitimate questions.
I would argue the onus is on the manufacturers and the health regulatory agencies and our governments to provide answers to these legitimate questions that many people have.
So as a consequence, I view it as my personal responsibility to highlight what these outstanding questions are for people and to do my best to provide fact-based assessments of their potential implications.
https://dryburgh.com/byram-bridle-coronavirus-vaccine-concerns/
Dr Jane Ruby – Myocarditis caused by mRNA coded spike protein injection
Myocarditis is an inflammation, it is an infection of the heart. It has long term complications for congestive heart failure and it is at the root of the cause of many blood clots and bleeding.
The CDC has been saying “It’s just a few cases and they’re looking into it” Well, they’ve known about this since Israel started reporting it in the middle of April. It’s more than a few cases. Israel reports that originally they thought it was about one in 50,000. It’s mostly young people and it’s now about 1700 cases. In Israel, per 50,000 that comes out to about one in 2500 and in the world of medicine, that’s a big number.
The bombshell that I want everybody to know, is that the FDA and the CDC and anybody else who’s paying attention to the literature knew on December 21st, 2020 that the spike proteins are responsible for cardiac damage.
We have scientific proof that it is dangerous for anyone who’s had the natural COVID infection to get these vaccines.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8011690/
Did Pfizer Fail to Perform industry Standard Animal Testing Prior to Initiation of mRNA Clinical Trials?
The Many Ways in Which COVID Vaccines May Harm Your Health
STORY AT-A-GLANCE
Analysis by Dr. Joseph Mercola
COVID-19 vaccines are capable of causing damage in a number of different ways. Disturbingly, all these different mechanisms of harm have synergistic effects when it comes to dysregulating your innate and adaptive immune systems and activating latent viruses.
The worst symptoms of COVID-19 are created by the SARS-CoV-2 spike protein, and that is the very thing gene-based COVID vaccines are instructing your body to make
While the natural spike protein is bad, the spike protein your body produces in response to the vaccine is even worse, as the synthetic RNA has been manipulated in such a way as to create a very robust and unnatural spike protein
The spike protein is toxic in and of itself, and has the ability to induce vascular, heart and neurological damage
The COVID-19 vaccine disables the Type I interferon pathway, which explains why vaccinated patients are reporting herpes and shingles infection following COVID-19 vaccination.
Is a Coronavirus Vaccine a Ticking Time Bomb?
Dr Doug Corrigan. – Ph.D. in Biochemistry and Molecular Biology, a master’s in Engineering Physics (concentration: Solid State Physics), and a bachelor’s in Engineering Physics (concentration: electrical engineering.)
Will a vaccine to SARS-CoV-2 actually make the problem worse? Although not a certainty, all of the current data says that this prospect is a real possibility that needs to be paid careful attention to. If you stay with me, I’ll explain why.
https://sciencewithdrdoug.com/2020/08/01/is-a-coronavirus-vaccine-a-ticking-time-bomb/
Prof. Dr Dolores Cahill Molecular Biologist, Immunologist
Immune system can save everyone from Covid-19; No one needs to die from Covid-19, flu symptoms can be avoided and the new mRNA vaccines are deadly.
So says molecular biologist and immunologist, Ph.D. Dolores Cahill, for Update, which we met at an event in Copenhagen, organized by the World Freedom Alliance.
Cahill is an international expert on the immune system and vaccines and has decades of research behind him.
In parallel, she has held a number of international top positions for e.g. for the European Commission. She tells in the interview which vitamins, minerals and preparations can save everyone from dying of Covid-19, reduce flu symptoms and provide security for the elderly with poor health.
Her warnings against the new mRNA vaccines cannot be overstated.
She would rather go to jail than be vaccinated with them, and if someone – against her will – gave her an injection, she would prosecute them for attempted murder.
Prior to May 2020, there were no approved mRNA vaccines, due to high mortality rates in the trials that may occur months or years after vaccination. According to Cahill, doctors, politicians and big-tech should be held directly and criminally accountable when they dissuade the population from vital information, prevention and proper treatment.
mRNA vaccines dangers – Dolores Cahill and Alexandra Henrion-Caude
Prof. Dr Dolores Cahill Molecular Biologist, Immunologist https://www.researchgate.net/profile/Dolores_Cahill
Alexandra Henrion-Caude, biomedical researcher.Patents for bioinformatic tool in microRNA field: MIRIFIX. Grantee, European, Inserm, French and Canada Association, 2001-2010. https://www.researchgate.net/profile/Alexandra_Henrion-Caude
Video starting at 8m:35s -Alexandra Henrion-Caude
The informed consent to be disclosed to any vaccine trial subjects, which is in fact any person who is currently being vaccinated. The risk of COVID-19 vaccines worsening clinical disease.
Especially given the response of the Th2 lymphocytes, a specific response that can take place in elderly! It is highly expected that elderly people will be more at risk actually of all the procedures
The conclusion leaves no place for interpretation! It is an ethical aspect that we should be raising! The specific and significant COVID19 vaccine risk of ADE (antibody dependent enhancement).
It should be prominently and independently disclosed to research subjects currently in vaccine trials as well as those being recruited for the trials and future patients after vaccine approval in order to meet the medical ethics standards of patient comprehension for informed consent.
Informed consent disclosure to vaccine trial subjects of risk of COVID-19 vaccines worsening clinical disease https://pubmed.ncbi.nlm.nih.gov/33113270/
Conclusions drawn from the study and clinical implications: The specific and significant COVID-19 risk of ADE should have been and should be prominently and independently disclosed to research subjects currently in vaccine trials, as well as those being recruited for the trials and future patients after vaccine approval, in order to meet the medical ethics standard of patient comprehension for informed consent.
Professor Dr Dolores Cahill Why people will start dying a few months after the 1st mRNA vaccinations
Professor Dr Dolores Cahill Explains “Immunization with SARS Coronavirus Vaccines Leads to Pulmonary Immunopathology on Challenge with the SARS Virus”
Acces the report on the NIH website via this link or download the saved copy below
Dr Wolfgang Wodarg Dec 3, 2020 – Concerns over the health and safety
Concerns over the health and safety of the human test subjects in Pfizer’s European COVID vaccine study have caused two eminent doctors to launch a petition calling for an immediate halt to those studies.
On December 1, 2020, Dr. Michael Yeadon, an ex chief of research at Pfizer and Dr. Wolfgang Wodarg, a lung specialist and former department head of public health lodged an appeal to the EMA, the European Medicine Agency responsible for approving drugs across the EU, asking them to suspend the ongoing Pfizer/BioNtech COVID vaccine study on BNT162b (EudraCT number 2020-002641-42).
https://lifepetitions.com/petition/halt-covid-vaccine-testing-in-europe
Dr. Mike Yeadon No need for vaccines, ‘the pandemic is effectively over’
Pfizer’s former Vice President and Chief Scientist for Allergy & Respiratory, states that the drive for a universal vaccine has ‘the whiff of evil’ which he ‘will oppose … vigorously.’
There is absolutely no need for vaccines to extinguish the pandemic. I’ve never heard such nonsense talked about vaccines. You do not vaccinate people who aren’t at risk from a disease. You also don’t set about planning to vaccinate millions of fit and healthy people with a vaccine that hasn’t been extensively tested on human subjects.
Dr. James Lyons-Weiler | PA Medical Freedom Press Conference
PA Medical Freedom Press Conference 10/20/20 – Opposing Covid vaccine mandates and medical care discrimination.
Research scientist James Lyons – Weiler, PhD, is President and CEO of The Institute for Pure and Applied Knowledge , Founder of IPAK-EDU.org, and the author of “Cures vs. Profits“, “Environmental and Genetic Causes of Autism“, and “Ebola:An Evolving Story” Dr. Lyons-
Weiler has been conducting biomedical research for over 20 years and has 58 peer-reviewed publications.
After earning a PhD in Ecology, Evolution & Conservation in Biology, he won an AP Sloan Postdoctoral Fellowship in Computational Molecular Biology at Pennsylvania State University.
Prior to founding IPAK and IPAK-EDU, he was a full faculty member at the University of Pittsburgh Cancer Institute, faculty in the Department of Pathology in the School and Medicine at the University of Pittsburgh, and Senior Research Scientist/Scientific Director of the University of Pittsburgh’s Bioinformatics Analysis Core in support of translational research, systems biology, sequence analysis, and the creation of novel algorithmic solutions for the analysis of complex and challenging data.
Prof. Francis Boyle -Do Not Take These Frankenshots!
Prof Boyle has some very strong statements about the Pfizer and Moderna mRNA vaccine.
Prof Boyle drafted the US domestic implementing legislation for the Biological Weapons Convention, known as the Biological Weapons Anti-Terrorism Act of 1989, that was approved unanimously by both Houses of the US Congress and signed into law by President George H.W. Bush.
I deliberately copied the above from his CV since he is drawing a direct parallel with the vaccination of US soldiers serving in the 1st Gulf war. He calls this war-crimes breaking the Nuremberg code with experiments on the vaccines for these soldiers. 500.000 troops inoculated, 11.000 were killed and 100,000 were disabled and those were healthy young men and women in US armed forces
Those experimental vaccines have been approved under the same emergency approval procedure as the COVID-19 vaccine.
Further more he states that COVID19 is an offensive biological warfare weapon Biosafety Level 4 laboratory (BSL-4) from which he believes the infectious disease escaped. Which is China’s equivalent to Fort Detrick and they have to wear moon suits and portable air supplies showing dangerous it is in these facilities. COVID-19 was developed not only at the Wuhan BSL 4 but also at the University of North Carolina bio safety Level 3 land. Doctor Shi Zhengli, the black Queen from Wuhan BSL 4 took a synthetic recombinant virus using synthetic biology making it more lethal and more infectious.
Prof Boyle is not the only scientist talking about a laboratory as the origin for the covid-19 virus. Prof. Luc Montagnier “Virus is Manipulated. A very Meticulous job”
Norwegian virologist Birger Sørensen “I firmly believe that it was spread by accident. When US authorities conducted an inspection in Wuhan in 2018, it was described as a risk lab.
More details on the main blog
The text below copied from Youtube. I saved the video because I don’t believe it will last long on Youtube.
Prof Boyle talks to Jason Liosatos warning us not to take to the Frankenshots and explains why
Support Jason’s work here https://www.patreon.com/JasonLiosatos
See my previous talks with Prof. Francis Boyle this year here:
Feb 2020 https://www.youtube.com/watch?v=5snzK…
March 2020 https://www.youtube.com/watch?v=L5rEm…
April 2020 https://www.youtube.com/watch?v=n2vGn…
Jason’s book and website: http://jasonliosatos.com/
See all Jason’s shows here https://www.youtube.com/user/GlobalPe…
Jason’s online art classes https://jasonliosatosartclasses.com/
Prof. Dr. Sucharit Bhakdi (Germany)
Interview with Laura Ingraham
December 2, 2020 – LAURA INGRAHAM (HOST): Doctor, on the issue of the vaccine, tonight, Anthony Fauci, on this network, actually said that 75 percent of Americans are going to have to get vaccinated to reach what they call “herd immunity”. Do you — do you buy that?
DR. SUCHARIT BHAKDI (GUEST): What utter nonsense. I know that Dr. Fauci is a renowned
HOST: —immunologist.
GUEST: medical scientist and immunologist. But what he says has to be wrong. And this is also what we have taken great lengths to explain in the book. And why — you know, someone who says this, has not the slightest inkling of the basics of immunology. And this is very, very surprising for someone of Dr. Fauci’s standing. And I would dare to defy him anywhere in the world at any time. But I cannot do this in 2 minutes.
INGRAHAM: Well, so you believe that the COVID vaccine is not necessary?
BHAKDI: I think it’s downright dangerous. And I warn you, if you go along these lines, you are going to go to your doom. And it’s so, so unnecessary.
Then the video ends abrupt because they don’t have more time ….
https://principia-scientific.com/book-review-corona-false-alarm-facts-and-figures
Book review in PDF form
Sucharit Bhakdi Warns Against Hastily Created Gene-Altering Coronavirus Vaccine (video)
In the following RAIR Foundation USA exclusively-translated video, German virologist Doctor Sucharit Bhakdi expresses deep suspicion of the vaccination development process in place for the Chinese coronavirus, which violates well-established scientific norms. The Doctor makes several very powerful points that should be considered by those touting a potential vaccine.
Open Letter from Doctors Scientists Regarding Covid Vaccine Safety
28 February 2021
Dear Sirs/Mesdames,
FOR THE URGENT PERSONAL ATTENTION OF: EMER COOKE, EXECUTIVE DIRECTOR OF THE EUROPEAN MEDICINES AGENCY
As physicians and scientists, we are supportive in principle of the use of new medical interventions which are appropriately developed and deployed, having obtained informed consent from the patient. This stance encompasses vaccines in the same way as therapeutics.
We note that a wide range of side effects is being reported following vaccination of previously healthy younger individuals with the gene-based COVID-19 vaccines. Moreover, there have been numerous media reports from around the world of care homes being struck by COVID-19 within days of vaccination of residents. While we recognise that these occurrences might, every one of them, have been unfortunate coincidences, we are concerned that there has been and there continues to be inadequate scrutiny of the possible causes of illness or death under these circumstances, and especially so in the absence of post-mortems examinations.
In particular, we question whether cardinal issues regarding the safety of the vaccines were adequately addressed prior to their approval by the European Medicines Agency (EMA).
Prof. Dr. Pierre Capel – Frikandel 3.0
Unfortunately this video is in the Dutch language without sub-titles
More from Professor emeritus http://www.pierrecapel.nl/ FOR THE JOY OF SCIENCE
Reverse transcription – Genome integration
Potential health risks of mRNA-based vaccine therapy: A hypothesis
K. Acevedo-Whitehouse, R. Bruno
Article 111015
https://www.sciencedirect.com/journal/medical-hypotheses/vol/171/suppl/C
Abstract
Therapeutic applications of synthetic mRNA were proposed more than 30 years ago, and are currently the basis of one of the vaccine platforms used at a massive scale as part of the public health strategy to get COVID-19 under control. To date, there are no published studies on the biodistribution, cellular uptake, endosomal escape, translation rates, functional half-life and inactivation kinetics of synthetic mRNA, rates and duration of vaccine-induced antigen expression in different cell types.
Furthermore, despite the assumption that there is no possibility of genomic integration of therapeutic synthetic mRNA, only one recent study has examined interactions between vaccine mRNA and the genome of transfected cells, and reported that an endogenous retrotransposon, LINE-1 is unsilenced following mRNA entry to the cell, leading to reverse transcription of full length vaccine mRNA sequences, and nuclear entry.
This finding should be a major safety concern, given the possibility of synthetic mRNA-driven epigenetic and genomic modifications arising.
We propose that in susceptible individuals, cytosolic clearance of nucleotide modified synthetic (nms-mRNAs) is impeded. Sustained presence of nms-mRNA in the cytoplasm deregulates and activates endogenous transposable elements (TEs), causing some of the mRNA copies to be reverse transcribed. The cytosolic accumulation of the nms-mRNA and the reverse transcribed cDNA molecules activates RNA and DNA sensory pathways. Their concurrent activation initiates a synchronized innate response against non-self nucleic acids, prompting type-I interferon and pro-inflammatory cytokine production which, if unregulated, leads to autoinflammatory and autoimmune conditions, while activated TEs increase the risk of insertional mutagenesis of the reverse transcribed molecules, which can disrupt coding regions, enhance the risk of mutations in tumour suppressor genes, and lead to sustained DNA damage. Susceptible individuals would then expectedly have an increased risk of DNA damage, chronic autoinflammation, autoimmunity and cancer. In light of the current mass administration of nms-mRNA vaccines, it is essential and urgent to fully understand the intracellular cascades initiated by cellular uptake of synthetic mRNA and the consequences of these molecular events.
https://www.sciencedirect.com/science/article/pii/S0306987723000117/pdfft?md5=534cf48210e10f01456b7fe6853c9aa3&pid=1-s2.0-S0306987723000117-main.pdf
Intracellular Reverse Transcription of Pfizer BioNTech COVID-19 mRNA Vaccine
https://www.mdpi.com/1467-3045/44/3/73
https://doi.org/10.3390/cimb44030073
Academic Editor: Stephen Malnick
Published: 25 February 2022
Abstract: Preclinical studies of COVID-19 mRNA vaccine BNT162b2, developed by Pfizer and BioNTech, showed reversible hepatic effects in animals that received the BNT162b2 injection.
Furthermore, a recent study showed that SARS-CoV-2 RNA can be reverse-transcribed and integrated into the genome of human cells. In this study, we investigated the effect of BNT162b2 on the human liver cell line Huh7 in vitro. Huh7 cells were exposed to BNT162b2, and quantitative PCR was performed on RNA extracted from the cells.
We detected high levels of BNT162b2 in Huh7 cells and changes in gene expression of long interspersed nuclear element-1 (LINE-1), which is an endogenous reverse transcriptase. Immunohistochemistry using antibody binding to LINE-1 open reading frame-1 RNA-binding protein (ORFp1) on Huh7 cells treated with BNT162b2 indicated increased nucleus distribution of LINE-1. PCR on genomic DNA of Huh7 cells exposed to BNT162b2 amplified the DNA sequence unique to BNT162b2. Our results indicate a fast up-take of BNT162b2 into human liver cell line Huh7, leading to changes in LINE-1 expression and distribution.
We also show that BNT162b2 mRNA is reverse transcribed intracellularly into DNA in as fast as 6 h upon BNT162b2 exposure.


Nov 2021 Warning – mRNA COVID Vaccines Dramatically Increase Endothelial Inflammatory Markers
Steven R Gundry – Originally published- 8 Nov 2021
mRNA COVID Vaccines Dramatically Increase Endothelial Inflammatory Markers and ACS Risk as Measured by the PULS Cardiac Test
Abstract
Our group has been using the PLUS Cardiac Test (GD Biosciences, Inc, Irvine, CA) a clinically validated measurement of multiple protein biomarkers which generates a score predicting the 5 yr risk (percentage chance) of a new Acute Coronary Syndrome (ACS).
The score has been measured every 3-6 months in our patient population for 8 years. Recently, with the advent of the mRNA COVID 19 vaccines (vac) by Moderna and Pfizer, dramatic changes in the PULS score became apparent in most patients. This report summarizes those results.
At the time of this report, these changes persist for at least 2.5 months post second dose of vac.
We conclude that the mRNA vacs dramatically increase inflammation on the endothelium and T cell infiltration of cardiac muscle and may account for the observations of increased thrombosis, cardiomyopathy, and other vascular events following vaccination. https://www.ahajournals.org/doi/abs/10.1161/circ.144.suppl_1.10712
Reverse-transcribed SARS-CoV-2 RNA can integrate into the genome of cultured human cells and can be expressed in patient-derived tissues
An unresolved issue of SARS-CoV-2 disease is that patients often remain positive for viral RNA as detected by PCR many weeks after the initial infection in the absence of evidence for viral replication. We show here that SARS-CoV-2 RNA can be reverse-transcribed and integrated into the genome of the infected cell and be expressed as chimeric transcripts fusing viral with cellular sequences.
We present here evidence that SARS-CoV-2 sequences can be reverse-transcribed and integrated into the DNA of infected human cells in culture. ….
These and other data are consistent with a target primed reverse transcription and retroposition integration mechanism and suggest that endogenous LINE1 RT can be involved in the reverse transcription and integration of SARS-CoV-2 sequences in the genomes of infected cells.
Our results may also be relevant for current clinical trials of antiviral therapies. If integration and expression of viral RNA are fairly common, reliance on extremely sensitive PCR tests to determine the effect of treatments on viral replication and viral load may not always reflect the ability of the treatment to fully suppress viral replication because the PCR assays may detect viral transcripts that derive from viral DNA sequences that have been stably integrated into the genome rather than infectious virus.
https://www.pnas.org/content/118/21/e2105968118
SARS-CoV-2 sequences transcribed in DNA detected in the genome of infected cells
Original article in German https://www.scinexx.de/news/medizin/coronavirus-dna-auch-in-unserem-erbgut read with Google translate
Surprising discovery: even though the coronavirus is an RNA virus, parts of its genome can be inserted into our DNA. This is proven by gene sequences of the virus in the DNA of cell cultures and in the tissues of Covid-19 patients.
Twitter comment from Pieter borger (MSc, PhD molecular genetics)
“Very interesting read. Every RNA molecule can potentially integrate in the genome because the two enzymes required to do so Reverse Transcriptase (RT) and integrase (INT) are 1000-fold present in our genome.”
Researchers led by Liguo Zhang from the Whitehead Institute for Biomedical Research in Cambridge have now investigated whether an infection with this virus can still leave genetic traces in the human genome. The impetus for this was provided by Covid patients whose PCR tests were still positive or positive again even months after the acute infection.
“We found copies of DNA from parts of the viral genome in almost all human chromosomes,” the team reports.”
SARS-CoV-2 spike protein can cause major damage to the walls of blood vessels.
“If you remove the replicating capabilities of the virus, it still has a major damaging effect on the vascular cells, simply by virtue of its ability to bind to this ACE2 receptor, the S protein receptor”
The paper, published on April 30, 2021, in Circulation Research, also shows conclusively that COVID-19 is a vascular disease, demonstrating exactly how the SARS-CoV-2 virus damages and attacks the vascular system on a cellular level. The findings help explain COVID-19’s wide variety of seemingly unconnected complications, and could open the door for new research into more effective therapies.
In the new study, the researchers created a “pseudovirus” that was surrounded by SARS-CoV-2 classic crown of spike proteins, but did not contain any actual virus. Exposure to this pseudovirus resulted in damage to the lungs and arteries of an animal model—proving that the spike protein alone was enough to cause disease.
COVID-19 RNA Based Vaccines and the Risk of Prion Disease
ABSTRACT
Development of new vaccine technology has been plagued with problems in the past. The current RNA based SARS- CoV-2 vaccines were approved in the US using an emergency order without extensive long term safety testing.
In this paper the Pfizer COVID-19 vaccine was evaluated for the potential to induce prion-based disease in vaccine recipients. The RNA sequence of the vaccine as well as the spike protein target interaction were analyzed for the potential to convert intracellular RNA binding proteins TAR DNA binding protein (TDP-43) and Fused in Sarcoma (FUS) into their pathologic prion conformations.
The results indicate that the vaccine RNA has specific sequences that may induce TDP-43 and FUS to fold into their pathologic prion confirmations. In the current analysis a total of sixteen UG tandem repeats (ΨGΨG) were identified and additional UG (ΨG) rich sequences were identified. Two GGΨA sequences were found. Potential G Quadruplex sequences are possibly present but a more sophisticated computer program is needed to verify these. Furthermore, the spike protein, created by the translation of the vaccine RNA, binds angiotensin converting enzyme 2 (ACE2), a zinc containing enzyme. This interaction has the potential to increase intracellular zinc. Zinc ions have been shown to cause the transformation of TDP-43 to its pathologic prion configuration. The folding of TDP-43 and FUS into their pathologic prion confirmations is known to cause ALS, front temporal lobar degeneration, Alzheimer’s disease and other neurological degenerative diseases.
The enclosed finding as well as additional potential risks leads the author to believe that regulatory approval of the RNA based vaccines for SARS-CoV-2 was premature and that the vaccine may cause much more harm than benefit.
https://scivisionpub.com/pdfs/covid19-rna-based-vaccines-and-the-risk-of-prion-disease-1503.pdf
36 COVID-19 vaccine recipients develop rare blood disorder after getting Moderna, Pfizer
This Side-Effect Is Not Age Or Gender Specific
Earlier this week, a report in the New York Times highlighted the fact that around 36 reports of this rare blood disorder, also called immune thrombocytopenia (ITP), was submitted to the federal government’s Vaccine Adverse Event Reporting System (VAERS).
A Florida physician has also reportedly died of the condition in January. The cases are equally divided between Pfizer and Moderna, manufacturers of the two COVID vaccines currently approved in the US, and they don’t seem to be age- or gender-specific. But experts are not very sure if the shots really did cause the problem, or if these people developed immune thrombocytopenia anyway. Some think that it is just a coincidence that symptoms surfaced post-vaccination.
https://www.thehealthsite.com/news/36-covid-19-vaccine-recipients-develop-rare-blood-disorder-after-getting-moderna-pfizer-shots-795552/
Rudolf Jaenisc – SARS-CoV-2 RNA reverse-transcribed and integrated into the human genome
Prolonged SARS-CoV-2 RNA shedding and recurrence of PCR-positive tests have been widely reported in patients after recovery, yet these patients most commonly are non-infectious1–14.
Here we investigated the possibility that SARS-CoV-2 RNAs can be reverse-transcribed and integrated into the human genome and that transcription of the integrated sequences might account for PCR-positive tests.
In support of this hypothesis, we found chimeric transcripts consisting of viral fused to cellular sequences in published data sets of SARS-CoV-2 infected cultured cells and primary cells of patients, consistent with the transcription of viral sequences integrated into the genome.
In this study, we showed evidence that SARS-CoV-2 RNAs can be reverse-transcribed and integrated into the human genome by several sources of reverse transcriptase such as activated human LINE-1 or co-infected retrovirus (HIV). We found LINE-1 expression can be induced upon SARS-CoV-2 infection or cytokine exposure, suggesting a molecular mechanism responsible for SARS-CoV-2 retro-integration in patients.
Moreover, our results suggest that the integrated SARS-CoV-2 sequences can be transcribed, as shown by RNA-Seq and smRNA-FISH data, providing a possible explanation for the presence of viral sequences at later times after initial virus exposure and in the absence of detectable infectious virus1–14.
Biography Rudolf Jaenisch; one of the co-writers in this study
Whitehead Institute for Biomedical Research, Cambridge, MA, USA Department of Biology, Massachusetts Institute of Technology, Cambridge, MA, USA
https://www.pnas.org/content/101/39/13982
https://www.biorxiv.org/content/10.1101/2020.12.12.422516v1
Study: SARS-CoV-2 RNA can be reverse-transcribed to be part of chimeric viral-human genome.
A study appearing as a preprint on the bioRxiv* server in December 2020 reveals that the genome of the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) is inserted into the human genome, accounting for the detection of viral RNAs, even in late convalescence.
Multiple cases of apparent reinfection have been reported over the past year. Though some have been rigorously investigated and found to be genuine cases of reinfection, evidenced by the presence of different strains of SARS-CoV-2 in the two episodes, it seems unlikely that this is the case with most. Additionally, no replication-competent virus has been isolated.
Implications and future directions
“Our results show induced LINE-1 expression in cells stressed by viral infection or exposed to cytokines, suggesting a molecular mechanism for SARS-CoV-2 retro-integration in human cells.”
- Chimeric reads present in published RNA sequences
- Sources of RT activity: LINE-1 or HIV-1
- N sequences found in the cell nucleus
- LINE-1 and cytokines mediate reverse transcription
Full article online:
https://www.news-medical.net/news/20201216/SARS-CoV-2-RNA-can-be-reverse-transcribed-to-be-part-of-chimeric-viral-human-genome.aspx
Informed consent disclosure to vaccine trial subjects of risk of COVID‐19 vaccines worsening clinical disease
Results of the study
COVID‐19 vaccines designed to elicit neutralising antibodies may sensitise vaccine recipients to more severe disease than if they were not vaccinated. Vaccines for SARS, MERS and RSV have never been approved, and the data generated in the development and testing of these vaccines suggest a serious mechanistic concern: that vaccines designed empirically using the traditional approach (consisting of the unmodified or minimally modified coronavirus viral spike to elicit neutralising antibodies), be they composed of protein, viral vector, DNA or RNA and irrespective of delivery method, may worsen COVID‐19 disease via antibody‐dependent enhancement (ADE). This risk is sufficiently obscured in clinical trial protocols and consent forms for ongoing COVID‐19 vaccine trials that adequate patient comprehension of this risk is unlikely to occur, obviating truly informed consent by subjects in these trials.
Conclusions drawn from the study and clinical implications
The specific and significant COVID‐19 risk of ADE should have been and should be prominently and independently disclosed to research subjects currently in vaccine trials, as well as those being recruited for the trials and future patients after vaccine approval, in order to meet the medical ethics standard of patient comprehension for informed consent.
1 THE RISK OF ADE IN COVID‐19 VACCINES IS NON‐THEORETICAL AND COMPELLING
2 CHALLENGES TO INFORMED CONSENT FOR COVID‐19 VACCINE STUDIES
3 CONCLUSION
Given the strong evidence that ADE is a non‐theoretical and compelling risk for COVID‐19 vaccines and the “laundry list” nature of informed consents, disclosure of the specific risk of worsened COVID‐19 disease from vaccination calls for a specific, separate, informed consent form and demonstration of patient comprehension in order to meet medical ethics standards. The informed consent process for ongoing COVID‐19 vaccine trials does not appear to meet this standard. While the COVID‐19 global health emergency justifies accelerated vaccine trials of candidates with known liabilities, such an acceleration is not inconsistent with additional attention paid to heightened informed consent procedures specific to COVID‐19 vaccine risks.
First published: 28 October 2020 https://doi.org/10.1111/ijcp.13795
Dr Doug -Will an RNA Vaccine Permanently Alter My DNA?
Posted by Dr. Doug Posted in COVID-19, vaccine
My professional opinion is that since RNA vaccines are a new mode of delivering vaccines, they should be tested for 5-10 years to demonstrate that genetic modification is not a major concern.
In addition, all coronavirus vaccines, regardless of type, should be tested for an equal duration to show that ADE is not a concern.
It is absolutely impossible to rule out these safety concerns in less than a year.
Antibody-dependent enhancement and SARS-CoV-2 vaccines and therapies
https://www.nature.com/articles/s41564-020-00789-5#Sec10
Data from the study of SARS-CoV and other respiratory viruses suggest that anti-SARS-CoV-2 antibodies could exacerbate COVID-19 through antibody-dependent enhancement (ADE). Previous respiratory syncytial virus and dengue virus vaccine studies revealed human clinical safety risks related to ADE, resulting in failed vaccine trials.
ADE has been observed in SARS, MERS and other human respiratory virus infections including RSV and measles, which suggests a real risk of ADE for SARS-CoV-2 vaccines and antibody-based interventions. However, clinical data has not yet fully established a role for ADE in human COVID-19 pathology. Steps to reduce the risks of ADE from immunotherapies include the induction or delivery of high doses of potent neutralizing antibodies, rather than lower concentrations of non-neutralizing antibodies that would be more likely to cause ADE.
Going forwards, it will be crucial to evaluate animal and clinical datasets for signs of ADE, and to balance ADE-related safety risks against intervention efficacy if clinical ADE is observed. Ongoing animal and human clinical studies will provide important insights into the mechanisms of ADE in COVID-19. Such evidence is sorely needed to ensure product safety in the large-scale medical interventions that are likely required to reduce the global burden of COVID-19.
Dr Peter Borger -The facts are that RNA vaccins can potentially change your DNA
The science facts are that RNA vaccins can potentially change your DNA. To understand how, we have to go a bit into genomics. Our genome contains about 50-60 thousand genes (~20 thousand protein-coding genes, the rest RNA genes). Together they make up about 25% of the genome.
In addition to that, our genome contains about 50% so called transposable and transposed elements (TEs), including ERVs and LINEs. The latter function, among other things, as (epi)genetic switches to control when genetic programs are switched on and off.
Interestingly, ERVs and LINEs both posses genes for the enzymes “reverse transcriptase (RT)” and “integrase” (INT). The RT enzyme converts RNA into cDNA, whereas the INT enzyme can put cDNA back into the genome. They prefer doing this with viral-like RNA molecules.
Further, RNA vaccins use viruses as their genetic backbones. RNA vaccins contain viral RNAs. With thousands of copies of RT and INT genes in our genomes there is ample opportunity to put any viral RNA back into our DNA. So, RNA vaccins are potentially “genotoxic”.
“Genotoxic” means that the “RNA–>cDNA–>genome integration” mechanism can lead to disturbed genetic control. In the long run, that may lead to genetic abberations and disease. It should be noted that RNA vaccins were not tested to exclude above described genotoxicy.
Above text copied from Tweet below
Dr Andrew Wakefield -Messenger RNA vaccine is actually genetic engineering
Explaining why by definition a RNA vaccine isn’t a vaccine at all.
What could possibly go wrong, the potential for this to go horribly wrong is enormous it’s never been used in humans before it’s never been tested out and yet it’s been rushed to market. No liability for vaccines so they can shortcuts safety studies they can rush to market they don’t mind because they’re not going to pay a price for it they don’t pick up the tab for the damage done. The full interview in a pdf for download below the video
And for those who would like to discredit Dr Andrew Wakefield listen to the video below:
Del Bigtree sets the record straight over Andrew Wakefield
An Evidence Based Perspective on mRNA-SARS-CoV-2 Vaccine Development
Although these beneficial features of mRNA vaccines provide some hope for the development of the first clinically applicable SARS-CoV-2 mRNA vaccine, recent reports regarding rare cases of moderate or severe reactions for different mRNA vaccines have raised concerns about safety and immunogenicity, including in the primary outcome findings of the phase I trial on mRNA-1273 [20,48]. Therefore, it is important to clearly understand the potential risks of this type of mRNA-based vaccine, which include local and systemic inflammatory responses, the biodistribution and persistence of the induced immunogen expression, possible development of autoreactive antibodies and toxic effects of any non-native nucleotides and delivery system components [48–50].
Therefore, it is important to clearly understand the potential risks of this type of mRNA-based vaccine, which include local and systemic inflammatory responses, the biodistribution and persistence of the induced immunogen expression, possible development of autoreactive antibodies and toxic effects of any non-native nucleotides and delivery system components [48–50].
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7218962/
Side effect, Adverse event
EudraVigilance – system for managing and analysing adverse reactions
Database links to the 4 main COVID-19 vaccinations
Moderna
Pfizer-BionTech
AstraZeneca
Janssen
https://www.adrreports.eu/en/eudravigilance.html
From 30 June 2022, it will be mandatory to report side effects to EudraVigilance using a data format based on international standards set by the International Organization for Standardization (ISO). This will help increase the data quality and analytical capabilities in EudraVigilance.
VAERS COVID Vaccine Myo/Pericarditis Reports
https://openvaers.com/covid-data/myo-pericarditis


The OpenVAERS Project:
VAERS is the Vaccine Adverse Event Reporting System put in place in 1990. It is a voluntary reporting system that has been estimated to account for only 1% ( see the Lazarus Report) of vaccine injuries. OpenVAERS is built from the HHS data available for download at vaers.hhs.gov.
The OpenVAERS Project allows browsing and searching of the reports without the need to compose an advanced search (more advanced searches can be done at medalerts.org or vaers.hhs.gov).
OpenVAERS is a private organization that posts publicly available CDC/FDA data of injuries reported post-vaccination. Reports are not proof of causality. https://openvaers.com/openvaers
Adverse Events Following SARS-CoV-2 mRNA Vaccination in Adolescents
December 2023 – A Norwegian Nationwide Register-Based Study.
doi: https://doi.org/10.1101/2023.12.13.23299926
Abstract
Background Vaccination of older adolescents against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) started in the spring of 2021 and continued with younger adolescents throughout the summer and fall. We assessed risks of adverse events following immunization (AEFI) in adolescents aged 12–19 years following SARS-CoV-2 vaccination with a messenger RNA (mRNA) vaccine in Norway.
Materials and Methods The study sample included 496,432 adolescents born in 2002–2009, residing in Norway, and unvaccinated against SARS-CoV-2 at the beginning of the age-specific waves of vaccination in 2021. The exposures under study were first- and second-dose SARS-CoV-2 mRNA vaccinations vs. no dose. We applied Poisson regression and self-controlled case series (SCCS) analysis to estimate incidence rate ratios (IRRs) of 17 preselected outcomes, with associated 95% confidence intervals (CIs), between vaccinated and unvaccinated subjects using predefined post-vaccination risk windows.
Results Most outcome-specific numbers of cases were low. There were no statistically significant associations between first-dose vaccination and any of the outcomes. In the main Poisson regression, second-dose vaccination was associated with increased risks of anaphylactic reaction (adjusted IRR [aIRR]: 10.05; 95% CI: 1.22–82.74), lymphadenopathy (aIRR: 2.33; 95% CI: 1.46–3.72), and myocarditis and pericarditis (aIRR: 5.27; 95% CI: 1.98–14.05). We also observed increased incidence of acute appendicitis outside the 14-day risk window. When expanding the risk window to 42 days in a post-hoc analysis, there was increased incidence of acute appendicitis following both first-dose vaccination (aIRR: 1.39; 95% CI: 1.09–1.78) and second-dose vaccination (aIRR: 1.43; 95% CI: 1.07–1.91). Results of the SCCS analysis were similar to the Poisson regression.
Conclusions In general, potential AEFI were rare among adolescents. We found increased risks of anaphylactic reaction, lymphadenopathy, and myocarditis and pericarditis following second-dose vaccination. There were also indications of increased acute appendicitis risk when applying longer risk windows.
‘Spikeopathy’: COVID-19 Spike Protein Is Pathogenic, from Both Virus and Vaccine mRNA
Biomedicines 2023, 11(8), 2287; https://doi.org/10.3390/biomedicines11082287
Submission received: 17 June 2023 / Revised: 17 July 2023 / Accepted: 24 July 2023 / Published: 17 August 2023
7. Evidence of ‘Spikeopathy’—Spike Protein Pathogenicity
The spike protein of SARS-CoV-2 has turned out to be pathogenic. The term “spikopathy” has been coined [98] as its pathological effects, like tuberculosis, appear to be legion, widespread in body organs, and induce a myriad of known diseases and syndromes. The term is spelled “spikeopathy” by others on the internet and we have chosen that spelling.
Figure 6 shows the FDA was aware of this potential before the public release of the gene-based COVID-19 vaccines. It is the 16th slide from a PowerPoint presentation of the “Vaccines and Related Biological Products Advisory Committee (VRBPAC) 22 October 2020, Meeting” [99]. What is striking is the predictive accuracy of these mostly neurological, cardiovascular, and autoimmune “possible adverse events” with those reported to VAERS and other global vaccine injury databases.

Figure 6. Slide 16 FDA’s VRBPAC meeting, Oct. 2022 [99].
The website www.react19.org lists as of June 2023 over 3400 published papers and case reports of COVID-19 vaccine harms under over twenty organ system and syndrome headings [100]. Here, we will review some key organ systems in relation to the pathogenic effects of the COVID-19 mRNA and adenovectorDNA-produced spike proteins….
9. Conclusions
In this narrative review, we have established the role of the SARS-CoV-2 spike protein, especially the S1 subunit, as pathogenic. It is also now apparent that widely biodistributed spike proteins, produced by mRNA and adenovectorDNA gene codes, induce a wide variety of diseases….
Systematic review of autopsy findings in deaths after COVID19 vaccination
Published July 6, 2023
The rapid development and widespread deployment of COVID-19 vaccines, combined with a high number of adverse event reports, have led to concerns over possible mechanisms of injury including systemic lipid nanoparticle (LNP) and mRNA distribution, spike protein-associated tissue damage, thrombogenicity, immune system dysfunction, and carcinogenicity. The aim of this systematic review is to investigate possible causal links between COVID-19 vaccine administration and death using autopsies and post-mortem analysis.
https://zenodo.org/records/8120771
List of supporting references used in vaccine harms debate speech
Andrew Bridgen
Member of Parliament for North West Leicestershire since 2010
Following my speech on vaccine harms in the House of Commons earlier this week the following list contains a list of supporting scientific references. The list was proactively sent to journalists immediately after my speech.
List of supporting references used in vaccine harms debate speech
https://www.andrewbridgen.com/news/list-supporting-references-used-vaccine-harms-debate-speech
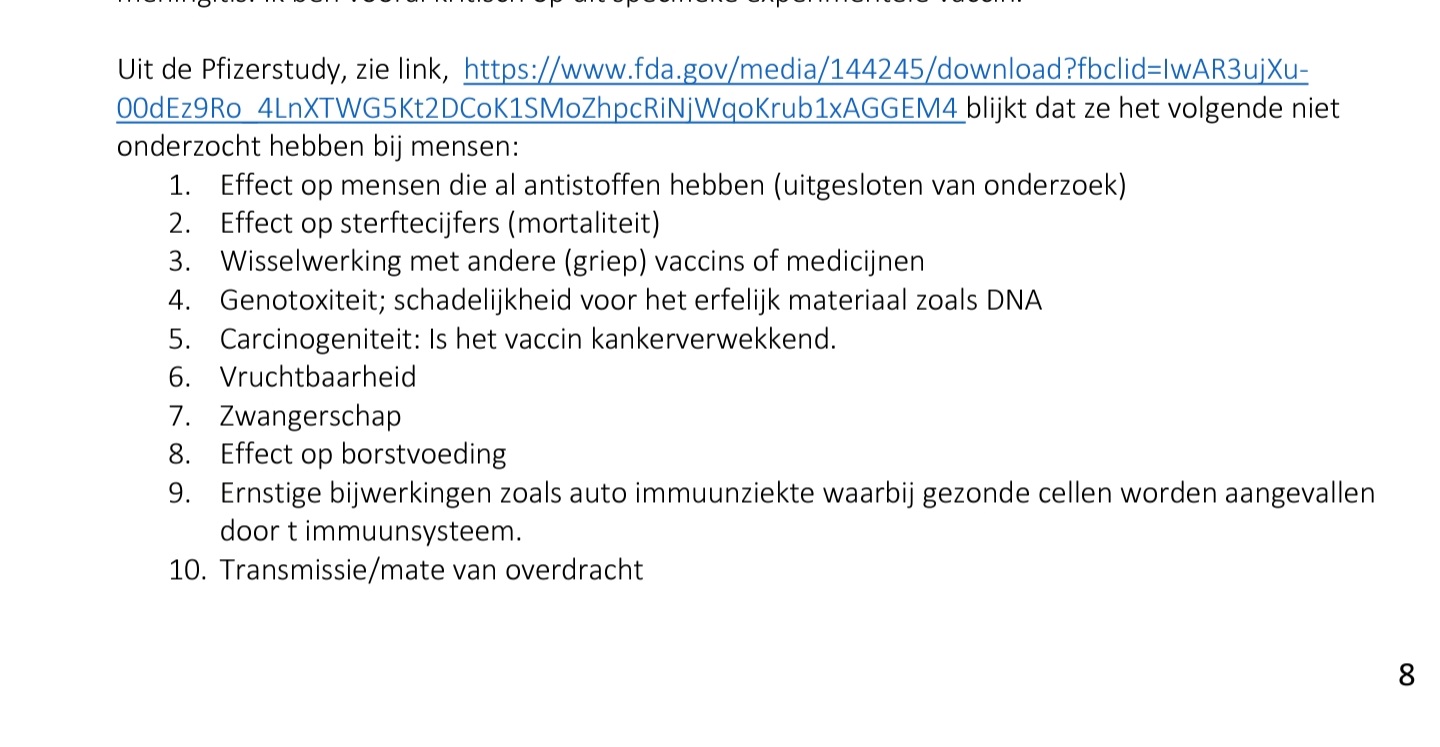{kind=link}
1250+ COVID Vaccine Publications and Case Reports
React19 is a science-based non-profit offering financial, physical, and emotional support for those suffering from longterm Covid-19 vaccine adverse events globally.
Mission
Our mission is to bring healing to the moms, dads, friends, and loved ones who are facing life-altering side effects from their Covid-19 vaccine. We build bridges between patients and research institutions in order to develop a better understanding of our vaccine complications.
https://react19.org/1250-covid-vaccine-reports/
Pfizer’s COVID-19 Vaccine Linked to Blood Clotting: FDA
Dec 2022 -Pfizer’s COVID-19 vaccine has been linked to blood clotting in older individuals, according to the U.S. Food and Drug Administration (FDA).
FDA researchers, crunching data from a database of elderly persons in the United States, found that pulmonary embolism—blood clotting that forms in the body and winds up blocking blood flow in the lungs—met the initial threshold for a statistical signal and continued meeting the criteria after a more in-depth evaluation.
Three other outcomes of interest—a lack of oxygen to the heart, a blood platelet disorder called immune thrombocytopenia, and another type of clotting called intravascular coagulation—initially raised red flags, researchers said. More in-depth evaluations, such as comparisons with populations who received influenza vaccines, showed those three as no longer meeting the statistical threshold for a signal.
Researchers looked at data covering 17.4 million elderly Americans who received a total of 34.6 million vaccine doses between Dec. 10, 2020, and Jan. 16, 2022.
The study was published by the journal Vaccine on Dec. 1.
https://www.theepochtimes.com/health/pfizers-covid-19-vaccine-linked-to-blood-clotting-fda_4930377.html
SARS-CoV-2 spike mRNA vaccine sequences circulate in blood up to 28 days after COVID-19 vaccination
Jan 17, 2023
In Denmark, vaccination against Severe Acute Respiratory Syndrome Corona Virus 2 (SARS-CoV-2) has been with the Pfizer-BioNTech (BTN162b2) or the Moderna (mRNA-1273) mRNA vaccines.
Patients with chronic hepatitis C virus (HCV) infection followed in our clinic received mRNA vaccinations according to the Danish roll-out vaccination plan.
To monitor HCV infection, RNA was extracted from patient plasma and RNA sequencing was performed on the Illumina platform.
In 10 of 108 HCV patient samples, full-length or traces of SARS-CoV-2 spike mRNA vaccine sequences were found in blood up to 28 days after COVID-19 vaccination. Detection of mRNA vaccine sequences in blood after vaccination adds important knowledge regarding this technology and should lead to further research into the design of lipid-nanoparticles and the half-life of these and mRNA vaccines in humans.
CDC Jul 2022 “Our cells break down mRNA from these vaccines and get rid of it within a few days”
https://pubmed.ncbi.nlm.nih.gov/36647776/
CDC July 2022 “Our cells break down mRNA from these vaccines and get rid of it within a few days“
Surveillance of COVID-19 vaccine safety among elderly persons aged 65 years and older
Risk of infection, hospitalisation, and death up to 9 months after a second dose of COVID-19 vaccine
The Lancet, arguably the most highly esteem medical journal, has released findings showing individuals, eight months after receiving their second vaccine dose, have immune systems that are notably suppressed relative to unvaccinated individuals
Summary
Background Vaccine effectiveness against COVID-19 beyond 6 months remains incompletely understood. We aimed to investigate the effectiveness of COVID-19 vaccination against the risk of infection, hospitalisation, and death during the first 9 months after vaccination for the total population of Sweden.
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(22)00089-7/fulltext
Fatal Multisystem Inflammatory Syndrome in Adult after SARS-CoV-2 Natural Infection and COVID-19 Vaccination
We describe a fatal case of multisystem inflammatory syndrome in an adult with onset 22 days after a second dose of mRNA coronavirus disease vaccine. Serologic and clinical findings indicated severe acute respiratory syndrome coronavirus 2 infection occurred before vaccination. The immunopathology of this syndrome, regardless of vaccination status, remains poorly understood.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8544993/
Adverse effects of COVID-19 vaccines and measures to prevent them
Abstract
Recently, The Lancet published a study on the effectiveness of COVID-19 vaccines and the waning of immunity with time. The study showed that immune function among vaccinated individuals 8 months after the administration of two doses of COVID-19 vaccine was lower than that among the unvaccinated individuals. According to European Medicines Agency recommendations, frequent COVID-19 booster shots could adversely affect the immune response and may not be feasible.
https://virologyj.biomedcentral.com/articles/10.1186/s12985-022-01831-05
Pfizer BNT162b2 – Cumulative Analysis of Post-authorization Adverse Event Reports
https://i-do-not-consent.netlify.app/media/5.3.6-postmarketing-experience.pdf
https://phmpt.org/wp-content/uploads/2021/11/5.3.6-postmarketing-experience.pdf
Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes, and MicroRNAs
The immune response to the vaccine is very different from that to a SARS-CoV-2 infection.
In this paper, we present evidence that vaccination induces a profound impairment in type I interferon signaling, which has diverse adverse consequences to human health.
Immune cells that have taken up the vaccine nanoparticles release into circulation large numbers of exosomes containing spike protein along with critical microRNAs that induce a signaling response in recipient cells at distant sites.
We also identify potential profound disturbances in regulatory control of protein synthesis and cancer surveillance.
These disturbances potentially have a causal link to neurodegenerative disease, myocarditis, immune thrombocytopenia, Bell’s palsy, liver disease, impaired adaptive immunity, impaired DNA damage response and tumorigenesis.
We show evidence from the VAERS database supporting our hypothesis.
https://pubmed.ncbi.nlm.nih.gov/35436552/

Increased emergency cardiovascular events among under-40 population

Published: Increased emergency cardiovascular events among under-40 population in Israel during vaccine rollout and third COVID-19 wave.
More recently, several studies established probable causal relationship between the messenger RNA (mRNA) vaccines of BNT162b2 and mRNA-127311,14,15,16 as well as adenovirus (ChAdOx1) vaccines17 with myocarditis, primarily in children, young and middle-age adults.
The study by the Ministry of Health in Israel, a country with one of the highest vaccination rates in the world, assesses the risk of myocarditis after receiving the 2nd vaccine dose to be between 1 in 3000 to 1 in 6000 in men of age 16–24 and 1 in 120,000 in men under 3011,12,13.
A follow up study by the US Center of Disease Control (CDC) based on the VAERS and V-Safe self-reporting systems18 further confirms these findings19.
The CDC has recently posted a warning regarding a vaccine-related risk of myocarditis, but still maintained their recommendation to vaccinate young individuals and children over 127.
Similar concerns are reflected in the recent Food and Drug Administration approval to the Pfizer vaccine that requires several follow studies on the short and long terms effects of myocarditis in young individuals20.
1,000 scientific studies on serious adverse effects of anti-Covid vaccines.
Professor Luc Montagnier, a virologist who was awarded the Nobel Prize in Medicine for the discovery of AIDS, was invited to the Luxembourg Parliament on Wednesday 12 January 2022 to speak about the vaccine. Geneticist Alexandra Henrion Caude was also present.
The video of Montagnier’s speech to the Luxembourg Parliament was hosted on You Tube but was deleted in less than a minute. Now the social media giants are apparently acting anti-democratically and in cooperation with Big Pharma and the governments.
The BNT162b2 mRNA vaccine against SARS-CoV-2 reprograms both adaptive and innate immune responses
June 2021 – The mRNA-based BNT162b2 vaccine from Pfizer/BioNTech was the first registered COVID-19 vaccine and has been shown to be up to 95% effective in preventing SARS-CoV-2 infections.
Little is known about the broad effects of the new class of mRNA vaccines, especially whether they have combined effects on innate and adaptive immune responses. Here we confirmed that BNT162b2 vaccination of healthy individuals induced effective humoral and cellular immunity against several SARS-CoV-2 variants. Interestingly, however, the BNT162b2 vaccine also modulated the production of inflammatory cytokines by innate immune cells upon stimulation with both specific (SARS-CoV-2) and non-specific (viral, fungal and bacterial) stimuli.
The response of innate immune cells to TLR4 and TLR7/8 ligands was lower after BNT162b2 vaccination, while fungi-induced cytokine responses were stronger.
In conclusion, the mRNA BNT162b2 vaccine induces complex functional reprogramming of innate immune responses, which should be considered in the development and use of this new class of vaccines.
https://www.medrxiv.org/content/10.1101/2021.05.03.21256520v1
https://www.medrxiv.org/content/10.1101/2021.05.03.21256520v1.full.pdf
Decoding COVID-19 mRNA Vaccine Immunometabolism in Central Nervous System
Posted March 02, 2022. doi: https://doi.org/10.1101/2022.03.02.482639
Abstract
The paper presents the effect of COVID-19 mRNA (Pfizer/BioNT) vaccine on in vitro glial cells of the brain studied by means of Raman spectroscopy and imaging.. The results obtained for human brain normal and tumor glial cells of astrocytes, astrocytoma, glioblastoma incubated with the Covid-19 mRNA vaccine Pfizer/BioNT vaccine show alterations in the reduction-oxidation pathways associated with Cytochrome c.
We found that the Pfizer/BioNT vaccine down regulate the concentration of cytochrome c in mitochondria upon incubation with normal and tumorous glial cells.
Concentration of oxidized form of cytochrome c in brain cells has been shown to decrease upon incubation the mRNA vaccine. Lower concentration of oxidized cytochrome c results in lower effectiveness of oxidative phosphorylation (respiration), reduced apoptosis and lessened ATP production. Alteration of Amide I concentration, which may reflect the decrease of mRNA adenine nucleotide translocator. Moreover, mRNA vaccine leads to alterations in biochemical composition of lipids that suggest the increasing role of signaling.
mRNA vaccine produce statistically significant changes in cell nucleus due to histone alterations.
The results obtained for mitochondria, lipid droplets, cytoplasm may suggest that COVID-19 mRNA (Pfizer/BioNT) vaccine reprograms immune responses.
The observed alterations in biochemical profiles upon incubation with COVID-19 mRNA in the specific organelles of the glial cells are similar to those we observe for brain cancer vs grade of aggressiveness.
New-onset autoimmune phenomena post-COVID-19 vaccination
First published: 27 December 2021 https://doi.org/10.1111/imm.13443
Recently, new-onset autoimmune phenomena after COVID-19 vaccination have been reported increasingly (e.g. immune thrombotic thrombocytopenia, autoimmune liver diseases, Guillain–Barré syndrome, IgA nephropathy, rheumatoid arthritis and systemic lupus erythematosus). Molecular mimicry, the production of particular autoantibodies and the role of certain vaccine adjuvants seem to be substantial contributors to autoimmune phenomena.
However, whether the association between COVID-19 vaccine and autoimmune manifestations is coincidental or causal remains to be elucidated. Here, we summarize the emerging evidence about autoimmune manifestations occurring in response to certain COVID-19 vaccines.
Dr Jessica Rose – FDA Public hearing Session
September 2021 – Vaccines and related Biological Products Advisory Committee
“There’s an over 1000% increase in the total number of adverse events just for 2021 and we are not done with 2021 … In my opinion [the risks] outweigh any potential benefits…with these products, especially in children.”
Myocarditis Adverse Events in VAERS in Association with COVID-19 Injectable Biological Products
October 1, 2021 – Following the global rollout and administration of the Pfizer Inc./BioNTech BNT162b2 and Moderna mRNA-1273 vaccines on December 17, 2020, in the United States, and of the Janssen Ad26.COV2.S product on April 1st, 2021, in an unprecedented manner, hundreds of thousands of individuals have reported adverse events (AEs) using the Vaccine Adverse Events Reports System (VAERS). We used VAERS data to examine cardiac AEs, primarily myocarditis, reported following injection of the first or second dose of the COVID-19 injectable products.
Myocarditis rates reported in VAERS were significantly higher in youths between the ages of 13 to 23 (p<0.0001) with ∼80% occurring in males. Within 8 weeks of the public offering of COVID-19 products to the 12-15-year-old age group, we found 19 times the expected number of myocarditis cases in the vaccination volunteers over background myocarditis rates for this age group.

As of May 18th, 2021, 600,000 children aged 12-15 had been injected with COVID-19 products3 .
The CDC estimated that 3,430,741 children aged 12-15 have received at least one dose of the COVID-19 products as of June 7th, 2021.
Since 1 per 100,000 children per year are affected by myocarditis then, statistically, we would expect ∼5 myocarditis cases if we calculate the expected number of cases using the June 7th CDC sample.
To date (up to and including July 2nd, 2021), 97 children aged 12-15 have had reports submitted to VAERS representing 17.4% of all myocarditis reports – and these are merely the cases that we are aware of. Thus, after 8 weeks of roll-out into the 12-15 years-old age group, we are at ∼19 times the expected number of cases within this sample.
Thus, the number of VAERS-reported cases far outnumber what would typically be expected to date. It is important to note that of the 559 myocarditis VAERS reports, 6 died (1.1%) and 33% of these deaths were in individuals under 20 years of age: 1 individual was 13 and one was 19 years of age. https://doi.org/10.1016/j.cpcardiol.2021.101011
Autopsy Histopathologic Cardiac Findings in Two Adolescents Following the Second COVID-19 Vaccine Dose
Feb 14, 2022
Context: – Myocarditis in adolescents has been diagnosed clinically following the administration of the second dose of an mRNA vaccine for coronavirus disease 2019 (COVID-19).
Objective: – To examine the autopsy microscopic cardiac findings in adolescent deaths that occurred shortly following administration of the second Pfizer-BioNTech COVID-19 dose to determine if the “myocarditis” described in these instances has the typical histopathology of myocarditis.
Design: – Clinical and autopsy investigation of two teenage boys who died shortly following administration of the second Pfizer-BioNTech COVID-19 dose.
Results: – The microscopic examination revealed features resembling a catecholamine-induced injury, not typical myocarditis pathology.
Conclusions: – The myocardial injury seen in these post-vaccine hearts is different from typical myocarditis and has an appearance most closely resembling a catecholamine-mediated stress (toxic) cardiomyopathy. Understanding that these instances are different from typical myocarditis and that cytokine storm has a known feedback loop with catecholamines may help guide screening and therapy.
https://pubmed.ncbi.nlm.nih.gov/35157759/
Severe Autoimmune Hemolytic Anemia Following Receipt of SARS-CoV-2 mRNA Vaccine
22 September 2021
Reports have emerged of autoimmune phenomena, including vaccine-associated myocarditis, immune thrombocytopenia, and immune thrombotic thrombocytopenia.
Here we present a novel case of a young woman who developed life-threatening autoimmune hemolytic anemia (AIHA) after her first dose of a SARS-CoV-2 mRNA vaccine.
https://onlinelibrary.wiley.com/doi/10.1111/trf.16672
(COVID-19) mRNA Vaccine Can Induce Acute Myopericarditis in Mouse Model
Post-vaccination myopericarditis is reported after immunization with coronavirus disease 2019 (COVID-19) messenger RNA (mRNA) vaccines. The effect of accidental intravenous injection of this vaccine on the heart is unknown.
This study provided in vivo evidence that inadvertent intravenous injection of COVID-19 mRNA vaccines may induce myopericarditis. Brief withdrawal of syringe plunger to exclude blood aspiration may be one possible way to reduce such risk.
https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciab707/6353927
Dr Malone, distribution of S-Protein throughout the body
Dr. Robert Malone, creator of mRNA vaccine technology:
The free Protein is a different story that comes out from Harvard and Brigham, and they did a a study of vaccinated nurses. So it’s pretty much an unimpeachable source! What that study showed, was that the vast majority had expression in circulation of free spike protein in their blood. They were all verified to not have been infected by SARS.-COV-2; it didn’t come from the virus. Infection came from vaccine !!
As somebody who spent a large fraction of their career trying to develop non viral gene therapy with both RNA and DNA. I was gobsmacked by the levels of protein, it appears that it’s a tip of the iceberg.
I’m sorry it didn’t work; we have a phenomena that we didn’t expect wasn’t predicted, but there it is. That’s the nature of science and evidence based medicine that we have to deal with it.
A dire warning from Dr. Charles Hoffe (blood clots)
A short summary of te video below:
We now know that only 25% of the injected mRNA actually stays in your arm and the other 75% is literally collected by your lymphatic system and fed into your circulation. So these little packages of messenger RNA, and by the way, in a single dose of a moderna vaccine, there are 40 trillion messenger RNA Molecules, 14 trillion that are injected into your arm. So 3/4 are taken by the lymphatics. Then go into your bloodstream. Obviously when something’s in circulation, the only cells that they’re going to get absorbed into is the cells around your blood vessels and the place where absorption happens is in the capillary networks.
The most alarming thing about this is that there are some parts of your body like your heart and your brain and your spinal cord and your lungs which cannot regenerate when those tissues are damaged, they are permanently damaged.
So on the basis of this D dimer test, which proves that the majority of people are clotting. These people, who now have reduced effort tolerance, literally what’s happened to them as they’ve plugged up thousands of tiny capillary’s in their lungs. The terrifying thing about this is not just that these people are now short of breath and can’t do what they used to be able to do, but once you block off a significant number of blood vessels through your lungs, your heart is now pumping up against a much greater resistance to try and get the blood through your lungs. And the problem that causes a condition called culinary artery hypertension. It’s like blood pressure, high blood pressure in your lungs because the blood can’t get through because so many of the vessels are blocked.
Like all these young people who are now getting myocarditis from these shots. They have permanently damaged hearts. It doesn’t matter how mild it is, they will not be able to do what they used to be able to do because heart muscle does not regenerate.
This is the terrifying concern and not only is the long term outlook very grim but with each successive shot, the damage will add and add. It’s going to be cumulative because you’re progressively getting more and more damaged.
Vaers reporting by the National Vaccine Information Center

Link to the Vaers reporting analysis
July 12, 2021 Janssen Biotech, Inc. letter to the FDA
Thrombosis with Thrombocytopenia
The reporting rate of thrombosis with thrombocytopenia following administration of the Janssen COVID-19 Vaccine has been highest in females ages 18 through 49 years; some have been fatal.
Guillain-Barré Syndrome
Reports of adverse events following use of the Janssen COVID-19 Vaccine under emergency use authorization suggest an increased risk of Guillain-Barré syndrome during the 42 days following vaccination.
OVERALL SAFETY SUMMARY
“Severe allergic reactions (including anaphylaxis), thrombosis with thrombocytopenia, Guillain-Barré syndrome, and capillary leak syndrome have been reported following administration of the Janssen COVID-19 Vaccine during mass vaccination outside of clinical trials.”
Temporal relation between 2nd dose BNT162b2 mRNA Covid-19 vaccine and cardiac involvement
Although these vaccines can counteract the COVID-19 pandemic, there is apprehension for patients who experienced previous SARS-COV-2 infection, as these subjects have not been tested in the trials [5]. Systemic reactogenicity, leading to systemic adverse events often occurred after dose 2 and within 2 days after vaccination [5]. The present report describes a case of cardiac involvement in a patient with previous SARS-COV-2 infection within days of the second dose of BNT162b2 mRNA vaccine.
An otherwise healthy 56-year-old man presented to the emergency department complaining of acute onset of chest pain 3 days after the second dose of BNT162b2 mRNA COVID-19 vaccine. He did not report fever, systemic symptoms or cutaneous rash after the first and second dose of the vaccine. He had no history of allergy. Nine months earlier he experienced mild signs of COVID-19 infection with fever lasting for 3 days and cough for 1 week, but he did not complain of chest pain or dyspnea. He was not hospitalized, and he took only acetaminophen. Nasopharyngeal swabs by real-time reverse-transcriptase–polymerase-chain-reaction (rRT-PCR) assay, had been persistently positive for 1 month while he did not undergo any blood tests during that period. One month later, anti-SARS-COV-2 serology demonstrated presence of IgG anti S1 and S2 proteins (titer of 60 AU/mL with positive threshold above 15).
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8011690/
COVID-19 vaccine AstraZeneca analysis print
All UK spontaneous reports received between 4/01/21 and /21 for COVID-19 vaccine Oxford University/AstraZeneca. 103 pages
Report Run Date: 13-May-2021
Data Lock Date: 12-May-2021 18:30:08

Side- and Adverse effects Articles December 2020
Dec 21: Suspicions grow that nanoparticles in Pfizer’s COVID-19 vaccine trigger rare allergic reactions
Severe allergy-like reactions in at least eight people who received the COVID-19 vaccine produced by Pfizer and BioNTech over the past 2 weeks may be due to a compound in the packaging of the messenger RNA (mRNA) that forms the vaccine’s main ingredient, scientists say. A similar mRNA vaccine developed by Moderna, which was authorized for emergency use in the United States on Friday, also contains the compound, polyethylene glycol (PEG). Full article online
Dec 20: CDC Issues New Guidelines, Launches Probe After 1000s Negatively-Affected Following COVID-19 Vaccination.
Thousands of people have been unable to work or perform daily activities, or required care from a healthcare professional, after getting the new COVID-19 vaccine, according to new data from the Centers for Disease Control and Prevention (CDC).
As of Dec. 18, 3,150 people reported what the agency terms “Health Impact Events” after getting vaccinated.
The definition of the term is: “unable to perform normal daily activities, unable to work, required care from doctor or health care professional.” Full article online.
Dec 19: FDA investigating five allergic reactions after Pfizer shot in U.S
Michael Erman NEW YORK (Reuters)
The U.S. Food and Drug Administration is investigating around five allergic reactions that happened after people were administered Pfizer Inc and BioNTech SE’s COVID-19 vaccine in the United States this week, a top FDA official said late on Friday.
Dr. Peter Marks, director of the FDA’s Center for Biologics Evaluation and Research, said at a press conference that the allergic reactions had been reported in more than one state, including in Alaska
Marks also said that a chemical called polyethylene glycol (PEG) that is an ingredient in the Pfizer vaccine – as well as the Moderna Inc vaccine authorized on Friday – “could be the culprit” causing the reactions.
Marks said that allergic reactions to PEG could be somewhat more common than previously understood. The cases in Alaska were similar to two cases reported last week in Britain.
Britain’s medical regulator has said that anyone with a history of anaphylaxis, or severe allergic reactions to a medicine or food, should not be given the Pfizer-BioNTech COVID-19 vaccine.
But the U.S. Food and Drug Administration has said that most Americans with allergies should be safe to receive the vaccine. It said only people who have previously had severe allergic reactions to vaccines or ingredients in this particular vaccine should avoid getting the shot.
On Friday, the FDA said the Moderna vaccine should not be given to individuals with a known history of a severe allergic reactions to any components of the shot.
The regulator is also requiring that appropriate medical treatments for immediate allergic reactions must be available when the shot is administered in case of an anaphylactic reaction.
Pfizer could not be immediately reached for comment.
Reporting by Michael Erman; Editing by Diane Craft and Daniel Wallis
https://www.reuters.com/article/us-health-coronavirus-vaccines-fda/fda-investigating-five-allergic-reactions-after-pfizer-shot-in-u-s-idUSKBN28T05J
Dec 16: Alaska healthcare worker with no history of drug allergies suffered serious ‘anaphylactic-like’ reaction
The worker allegedly had no history of allergies to any medication but it’s unknown if he or she had any other allergies.
The allergic reaction is believed to be similar to the anaphylactic-like reactions suffered by two healthcare workers in Great Britain, both whom have since recovered, after they were given the Pfizer-BioNTech SE vaccine.
https://www.dailymail.co.uk/health/article-9060697/Alaska-healthcare-worker-suffered-allergic-reaction-Pfizers-coronavirus-vaccine.html
Dec 12: French Expert Shocked By Number Of Adverse Reactions To COVID-19 Vaccine
“Not only is there a lack of information, but these injections based on genetic material (messenger RNA) have never passed the commercialization stage until now,” Caumes said. “Perhaps they are revolutionary, but I want proof of their reliability, otherwise it is tantamount to placing blind trust in industry.”
https://principia-scientific.com/french-expert-shocked-by-number-of-adverse-reactions-to-covid-19-vaccine/
Dec 10: As the United Kingdom started inoculating people with the coronavirus vaccine developed by Pfizer-BioNTech, four volunteers who were administered the vaccine in the trial stage developed Bell’s palsy, according to US Food and Drug Administration (FDA) regulators. Bell’s palsy is a form of temporary facial paralysis.
https://zeenews.india.com/world/covid-19-four-pfizer-vaccine-volunteers-develop-bells-palsy-read-details-here-2329924.html
UK Government officials are calling for calm after it emerged that several health workers have suffered an “anaphylactoid reaction” after receiving the Pfizer COVID-19 vaccine.British scientists attempted to quash public panic about the Pfizer/BioNTech following reports that two NHS staff suffered an adverse reaction just after being immunized this week.
https://neonnettle.com/news/13530-uk-health-workers-suffer-anaphylactoid-reaction-after-pfizer-s-covid-19-vaccine
Pfizer BioNtech Study: Vaccine has adverse event risks.
One cannot stress how untested this vaccine is. How the FDA would approve this against the known risks of COVID-19, which are very low (under 0.2%), but for a specific population with comorbidity issues that impact them for every flu season (approximately 5%). These people are, in totality, over 55, that have been most impacted (90%+ of U.S. Deaths).
https://dcfpress.com/pfizer-biontech-study-vaccine-has-adverse-events-risks/
Dec 9: Six people died in Pfizer’s late-stage trial of the COVID-19 vaccine, the US Food and Drug Administration has revealed just hours after Britain became the first country in the world to roll out the vaccine.
https://thenewdaily.com.au/news/coronavirus/2020/12/09/pfizer-oxford-astrazeneca-vaccines/
BOMBSHELL: More Death and Fever from Pfizer Vaccine than Covid
The FDA briefing document on the Pfizer-BioNTech COVID-19 vaccine contains some stunning information, including the revelation that most people are hundreds of times more likely to have an adverse reaction from their vaccine than they are to die from covid.
On Page 41 of the report, we can see a description of the Serious Adverse Events including 6 deaths and 12 cases of appendicitis. In total 0.6% of participants reported a Serious Adverse Events from the Covid Vaccine – 100 TIMES HIGHER THAN THE PROBABILITY OF DEATH FROM COVID (for under 60’s)
https://axisworldnews.com/2020/12/09/bombshell-more-die-from-vaccine-in-pfizer-trial-than-from-covid/
Dec 8: COVID-19 vaccine trial participants said they experienced intense symptoms and warned of possible “adverse effects” as novel coronavirus cases continue to surge across the U.S.
The U.S. Food and Drug Administration released a report Tuesday that said Pfizer and BioNTech’s COVID-19 vaccine candidate is safe and effective against the virus. The FDA also noted that while side effects were common, they have yet to identify the Pfizer vaccine’s safety concerns.
https://www.ibtimes.com/coronavirus-vaccine-side-effects-trial-participants-warn-intense-symptoms-possible-3097884
mRNA vaccines — a new era in vaccinology
Nature Reviews Drug Discovery volume 17, 261–279(2018)
Potential safety concerns that are likely to be evaluated in future preclinical and clinical studies include local and systemic inflammation, the biodistribution and persistence of expressed immunogen, stimulation of auto-reactive antibodies and potential toxic effects of any non-native nucleotides and delivery system components.
A possible concern could be that some mRNA-based vaccine platforms54,166 induce potent type I interferon responses, which have been associated not only with inflammation but also potentially with autoimmunity167,16.
Thus, identification of individuals at an increased risk of autoimmune reactions before mRNA vaccination may allow reasonable precautions to be taken.
Conclusions
While preclinical studies have generated great optimism about the prospects and advantages of mRNA-based vaccines, two recent clinical reports have led to more tempered expectations22,91. In both trials, immunogenicity was more modest in humans than was expected based on animal models, a phenomenon also observed with DNA-based vaccines171, and the side effects were not trivial.
https://www.nature.com/articles/nrd.2017.243
Transplacental Transmission of the COVID-19 Vaccine mRNA
Evidence from Placental, Maternal and Cord Blood Analyses Post-Vaccination.
Accepted Date: 24 January 2024
Lin X, Botros B, Hanna M, Gurzenda E, Manzano De Mejia C, Chavez M, Hanna N, “Transplacental Transmission of the COVID-19 Vaccine mRNA: Evidence from Placental,
Maternal and Cord Blood Analyses Post-Vaccination”, American Journal of Obstetrics and Gynecology (2024), doi: https://doi.org/10.1016/j.ajog.2024.01.022
Our findings suggest that the vaccine mRNA is not localized to the injection site and can spread 100 systemically to the placenta and umbilical cord blood.
The detection of the spike protein in the 101 placental tissue indicates the bioactivity of the vaccine mRNA reaching the placenta. Notably, the 102 vaccine mRNA was largely fragmented in the cord blood and, to a lesser extent, in the placenta. 103 To our knowledge, these two cases demonstrate, for the first time, the ability of the COVID-19 104 vaccine mRNA to penetrate the fetal-placental barrier and reach the intrauterine environment.
In a Twist, Scientists Find Cancer Drivers Hiding in RNA, Not DNA
2 Articles …
1) the original publication from 2018 – the Sloan Kettering Institute
Researchers at the Sloan Kettering Institute have found that changes in an information-carrying molecule called messenger RNA can inactivate tumor-suppressing proteins and thereby promote cancer. The findings pinpoint previously unknown drivers of the disease.
https://www.mskcc.org/news/scientists-find-cancer-drivers-hiding-rna-not-dna
2) Sceptic article from Naturalnews alarming the effect mRNA vaccination
MEDICAL SHOCKER: Scientists at Sloan Kettering discover mRNA inactivates tumor-suppressing proteins, meaning it can promote cancer.
After your Covid vaccination, RNA is transported out of your cell’s nucleus, and will no longer function properly as a cancer tumor suppressor
Widespread intronic polyadenylation inactivates tumour suppressor genes in leukaemia
DNA mutations are known cancer drivers. Here we investigated whether mRNA events that are upregulated in cancer can functionally mimic the outcome of genetic alterations.
RNA sequencing or 3′-end sequencing techniques were applied to normal and malignant B cells from 59 patients with chronic lymphocytic leukaemia (CLL)1,2,3.
We discovered widespread upregulation of truncated mRNAs and proteins in primary CLL cells that were not generated by genetic alterations but instead occurred by intronic polyadenylation. Truncated mRNAs caused by intronic polyadenylation were recurrent (n = 330) and predominantly affected genes with tumour-suppressive functions. The truncated proteins generated by intronic polyadenylation often lack the tumour-suppressive functions of the corresponding full-length proteins (such as DICER and FOXN3), and several even acted in an oncogenic manner (such as CARD11, MGA and CHST11). In CLL, the inactivation of tumour-suppressor genes by aberrant mRNA processing is substantially more prevalent than the functional loss of such genes through genetic events. We further identified new candidate tumour-suppressor genes that are inactivated by intronic polyadenylation in leukaemia and by truncating DNA mutations in solid tumours4,5.
These genes are understudied in cancer, as their overall mutation rates are lower than those of well-known tumour-suppressor genes. Our findings show the need to go beyond genomic analyses in cancer diagnostics, as mRNA events that are silent at the DNA level are widespread contributors to cancer pathogenesis through the inactivation of tumour-suppressor genes.
https://www.nature.com/articles/s41586-018-0465-8
Natural Immunity – Had COVID? You’ll probably make antibodies for a lifetime
Natural immunity to SARS-CoV-2 (obtained by infection) and vaccine-generated immunity to SARS-CoV2 are two different paths to immunity.
20+ studies on this page
Antibody Evolution after SARS-CoV-2 mRNA Vaccination
We conclude that memory antibodies selected over time by natural infection have greater potency and breadth than antibodies elicited by vaccination.
These results suggest that boosting vaccinated individuals with currently available mRNA vaccines would produce a quantitative increase in plasma neutralizing activity but not the qualitative advantage against variants obtained by vaccinating convalescent individuals.
https://www.biorxiv.org/content/10.1101/2021.07.29.454333v1
Covid-19 vaccine efficacy and effectiveness
Worldwide Bayesian Causal Impact Analysis of Vaccine
November 15, 2021
Worldwide Bayesian Causal Impact Analysis of Vaccine Administration on Deaths and Cases Associated with COVID-19: A BigData Analysis of 145 Countries
Policy makers and mainstream news anchors have promised the public that the COVID-19 vaccine rollout worldwide would reduce symptoms, and thereby cases and deaths associated with COVID-19. While this vaccine rollout is still in progress, there is a large amount of public data available that permits an analysis of the effect of the vaccine rollout on COVID-19 related cases and deaths. Has this public policy treatment produced the desired effect?
The statistically significant and overwhelmingly positive causal impact after vaccine deployment on the dependent variables total deaths and total cases per million should be highly worrisome for policy makers. They indicate a marked increase in both COVID-19 related cases and death due directly to a vaccine deployment that was originally sold to the public as the “key to gain back our freedoms.” The effect of vaccines on total cases per million and its low positive association with total vaccinations per hundred signifies a limited impact of vaccines on lowering COVID-19 associated cases. These results should encourage local policy makers to make policy decisions based on data, not narrative, and based on local conditions, not global or national mandates. These results should also encourage policy makers to begin looking for other avenues out of the pandemic aside from mass vaccination campaigns.
https://vector-news.github.io/editorials/CausalAnalysisReport_html.html
Effectiveness of the Coronavirus Disease 2019 (COVID-19) Bivalent Vaccine
The association of increased risk of COVID-19 with higher numbers of prior vaccine doses in our study, was unexpected.
A simplistic explanation might be that those who received more doses were more likely to be individuals at higher risk of COVID-19. A small proportion of individuals may have fit this description. However, the majority of subjects in this study were generally young individuals and all were eligible to have received at least 3 doses of vaccine by the study start date, and which they had every opportunity to do.
Therefore, those who received fewer than 3 doses (>45% of individuals in the study) were not those ineligible to receive the vaccine, but those who chose not to follow the CDC’s recommendations on remaining updated with COVID-19 vaccination, and
one could reasonably expect these individuals to have been more likely to have exhibited higher risk taking behavior.
Despite this, their risk of acquiring COVID-19 was lower than those who received a larger number of prior vaccine doses.
This is not the only study to find a possible association with more prior vaccine doses and higher risk of COVID-19. A

https://www.medrxiv.org/content/10.1101/2022.12.17.22283625v1.full.pdf
Three studies published by the CDC, British government & Oxford University conclude that Covid-19 Vaccines do not work
September 9, 2021 Nina Pierpont, MD, PhD
Covid-19 vaccines do not keep people from catching the prevailing Delta variant and passing it to others
- Excellent scientific research papers published or posted in August 2021 clearly demonstrate that current vaccines do not prevent transmission of SARS-CoV-2.
- Vaccines aim to achieve two ends:
- To protect the vaccinated person against the illness.
- To keep people from carrying the infection and transmitting it to others.
- If enough people are vaccinated or otherwise become immune, it is hoped that thedisease will stop circulating. We call this herd immunity.
- On the way to herd immunity, there is an assumption that people who are immunized canform safe clusters or groups within which no one is carrying or transmitting the virus.
- Unfortunately, this last assumption (2.b.ii) is no longer true under the new variant of SARS-CoV- 2, Delta( B.1.617.2), which now accounts for essentially all cases worldwide.
- Delta is more infectious than the Alpha strain (B.1.1.7) that prevailed in the UK from January to May 2021 (and in the US from March to June 2021), meaning that Delta is passed more readily person-to-person than the previous dominant strain.
– Infectiousness is a correlate of high viral load (see section 5, below).
– From its origin in India, Delta has soared to nearly complete domination of COVID-19 viral strains everywhere in a matter of months, because it spreads so easily and infects both vaccinated and unvaccinated people.
- New research in multiple settings shows that Delta produces very high viral loads (meaning, the densityof virus on a nasopharyngeal swab as interpreted from PCR cycle threshold numbers).
- Viral loads are much higher in people infected with Delta than they were in people infected withAlpha.
- Viral loads with Delta are equally high whether the person has been vaccinated or not.
- Viral load is an indicator of infectiousness. [13,14] The more virus one has in the nose and mouth, the more likely it is to be in this individual’s respiratory droplets and secretions, and tospread to others.
- Due to evolution of the virus itself, all the currently licensed vaccines (all based on the original Wuhanstrain spike protein sequence) have lost their ability to accomplish vaccine purpose 2(b), above, “To keeppeople from carrying the infection and transmitting it to others.”
- Vaccine mandates are thus stripped of their justification, since to vaccinate an individual no longerstops or even slows his ability to acquire and transmit the virus to others
- Under Delta, natural immunity is much more protective than vaccination. All severities of COVID-19 illness produce healthy levels of natural immunity.
Increases in COVID-19 are unrelated to levels of vaccination across 68 countries and 2947 counties in the United States
September 2021
Vaccines currently are the primary mitigation strategy to combat COVID-19 around the world.
For instance, the narrative related to the ongoing surge of new cases in the United States (US) is argued to be driven by areas with low vaccination rates [1].
A similar narrative also has been observed in countries, such as Germany and the United Kingdom [2].
At the same time, Israel that was hailed for its swift and high rates of vaccination has also seen a substantial resurgence in COVID-19 cases [3].
We investigate the relationship between the percentage of population fully vaccinated and new COVID-19 cases across 68 countries and across 2947 counties in the US.

At the country-level, there appears to be no discernable relationship between percentage of population fully vaccinated and new COVID-19 cases in the last 7 days (Fig. 1).
In fact, the trend line suggests a marginally positive association such that countries with higher percentage of population fully vaccinated have higher COVID-19 cases per 1 million people.
Notably, Israel with over 60% of their population fully vaccinated had the highest COVID-19 cases per 1 million people in the last 7 days.
The lack of a meaningful association between percentage population fully vaccinated and new COVID-19 cases is further exemplified, for instance, by comparison of Iceland and Portugal.
Both countries have over 75% of their population fully vaccinated and have more COVID-19 cases per 1 million people than countries such as Vietnam and South Africa that have around 10% of their population fully vaccinated.
https://link.springer.com/article/10.1007/s10654-021-00808-7
Nosocomial outbreak caused by the SARS-CoV-2 Delta variant in a highly vaccinated population, Israel, July 2021
We present an investigation of a coronavirus disease (COVID-19) outbreak that started from one unidentified COVID-19 patient, with extensive, rapid nosocomial spread among vaccinated, including individuals wearing surgical masks.
Discussion ” … all transmissions between patients and staff occurred between masked and vaccinated individuals … “
Conclusion “This nosocomial outbreak exemplifies the high transmissibility of the SARS-CoV-2 Delta variant among twice vaccinated and masked individuals… “
https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2021.26.39.2100822
Is the Pfizer vaccine as effective as claimed?
May 17, 2021 Norman Fenton and Martin Neil
There are, however, issues with the study and its analysis which mean the 95% effectiveness measure is exaggerated. In this article Will Jones argues that the researchers have not adjusted for the declining infection rate during the study period and that when you do so, the effectiveness drops to 74% (in the over 65’s).
https://wherearethenumbers.substack.com/p/important-caveats-to-pfizer-vaccine
The elephant (not) in the room
COVID-19 vaccine efficacy and effectiveness—the elephant (not) in the room
Lancet Microbe April 20, 2021 https://doi.org/10.1016/ S2666-5247(21)00069-0
Excerpts of these results have been widely communicated and debated through press releases and media, sometimes in misleading ways. Although attention has focused on vaccine efficacy and comparing the reduction of the number of symptomatic cases, fully understanding the efficacy and effectiveness of vaccines is less straightforward than it might seem. Depending on how the effect size is expressed, a quite different picture might emerge.

The lower the NNV and the higher the RRR, the better the vaccine efficacy. Details are in the appendix (p 3). RRR=relative risk reduction. NNV=numbers needed to vaccinate. NIH=US National Institutes of Health.
Although the relative risk reduction (RRR) considers only participants who could benefit from the vaccine, the absolute risk reduction (ARR), which is the difference between attack rates with and without a vaccine, considers the whole population.
ARRs tend to be ignored because they give a much less impressive effect size than RRRs:
- 1.3% for the AstraZeneca–Oxford
- 1.2% for the Moderna–NIH
- 1.2% for the J&J
- 0.93% for the Gamaley
- 0.84% for the Pfizer–BioNTech vaccines
Outcome Reporting Bias in COVID-19 mRNA Vaccine Clinical Trials
Received: 13 January 2021 / Revised: 15 February 2021 / Accepted: 22 February 2021 / Published: 26 February 2021
Abstract
Relative risk reduction and absolute risk reduction measures in the evaluation of clinical trial data are poorly understood by health professionals and the public.
The absence of reported absolute risk reduction in COVID-19 vaccine clinical trials can lead to outcome reporting bias that affects the interpretation of vaccine efficacy.
The present article uses clinical epidemiologic tools to critically appraise reports of efficacy in Pfzier/BioNTech and Moderna COVID-19 mRNA vaccine clinical trials.
Based on data reported by the manufacturer
For Pfzier/BioNTech vaccine BNT162b2, this critical appraisal shows:
relative risk reduction, 95.1%; 95% CI, 90.0% to 97.6%; p = 0.016;
absolute risk reduction, 0.7%; 95% CI, 0.59% to 0.83%; p < 0.000.
For the Moderna vaccine mRNA-1273, the appraisal shows:
relative risk reduction, 94.1%; 95% CI, 89.1% to 96.8%; p = 0.004;
absolute risk reduction, 1.1%; 95% CI, 0.97% to 1.32%; p < 0.000.
Unreported absolute risk reduction measures of 0.7% and 1.1% for the Pfzier/BioNTech and Moderna vaccines, respectively, are very much lower than the reported relative risk reduction measures.
Reporting absolute risk reduction measures is essential to prevent outcome reporting bias in evaluation of COVID-19 vaccine efficacy.
Conclusions
A critical appraisal of phase III clinical trial data for the Pfizer/BioNTech vaccine BNT162b2 and Moderna vaccine mRNA-1273 shows that absolute risk reduction measures are very much lower than the reported relative risk reduction measures.
Yet, the manufacturers failed to report absolute risk reduction measures in publicly released documents.
As well, the U.S FDA Advisory Committee (VRBPAC) did not follow FDA published guidelines for communicating risks and benefits to the public, and the committee failed to report absolute risk reduction measures in authorizing the BNT162b2 and mRNA-1273 vaccines for emergency use.
Such examples of outcome reporting bias mislead and distort the public’s interpretation of COVID-19 mRNA vaccine efficacy and violate the ethical and legal obligations of informed consent. https://www.mdpi.com/1648-9144/57/3/199/htm
Pfizer Covid-19 vaccine candidate is unimpressive: NNTV is around 256
Pfizer’s vaccine “may be more than 90% effective.” (Mahase, BMJ 2020;371:m4347, November 9)
Specific data are not given but it is easy enough to approximate the numbers involved, based on the 94 cases in a trial that has enrolled about 40,000 subjects: 8 cases in a vaccine group of 20,000 and 86 cases in a placebo group of 20,000.
This yields a Covid-19 attack rate of 0.0004 in the vaccine group and 0.0043 in the placebo group. Relative risk (RR) for vaccination = 0.093, which translates into a “vaccine effectiveness” of 90.7% [100(1-0.093)]. This sounds impressive, but the absolute risk reduction for an individual is only about 0.4% (0.0043-0.0004=0.0039).
The Number Needed To Vaccinate (NNTV) = 256 (1/0.0039), which means that to prevent just 1 Covid-19 case 256 individuals must get the vaccine; the other 255 individuals derive no benefit, but are subject to vaccine adverse effects, whatever they may be and whenever we learn about them
https://www.bmj.com/content/371/bmj.m4347/rr-4
Peter Doshi: Pfizer and Moderna’s “95% effective” vaccines—let’s be cautious and first see the full data
Let’s put this in perspective.
– First, a relative risk reduction is being reported, not absolute risk reduction, which appears to be less than 1%.
– Second, these results refer to the trials’ primary endpoint of covid-19 of essentially any severity, and importantly not the vaccine’s ability to save lives, nor the ability to prevent infection, nor the efficacy in important subgroups (e.g. frail elderly). Those still remain unknown.
– Third, these results reflect a time point relatively soon after vaccination, and we know nothing about vaccine performance at 3, 6, or 12 months, so cannot compare these efficacy numbers against other vaccines like influenza vaccines (which are judged over a season).
– Fourth, children, adolescents, and immunocompromised individuals were largely excluded from the trials, so we still lack any data on these important populations.
Covid Vaccines: The Good, The Bad, The Ugly
Updated: July 27, 2021 – Check the link for updates to this article
Published: July 23, 2021
New data from Hebrew University shows that protection against severe disease has already dropped to 80%; compared to the original 96%, this results in a five-fold increase in residual risk.
New data from Israel shows that 80% of fully vaccinated people haven’t infected others in public spaces. While authorities claim that this is a good result, in reality, it is not any different from unvaccinated people, thus confirming zero effectiveness against infection and transmission.
Thus, vaccine protection even against severe disease will likely further decrease due to new variants, or, in the very worst case, will turn into antibody-dependent disease enhancement (ADE), if high levels of non-neutralizing antibodies aggravate the infection. Indeed, this is what happened in the case of vaccines against SARS-1 and dengue fever.
However, there is a very real risk that additional vaccinations, which inject or induce the coronavirus spike protein, could substantially increase the risk of serious cardiovascular and neurological adverse events, such as strokes, GBS and heart muscle inflammation. Globally, covid vaccines may already have killed tens of thousands of people. Alternatives include safer oral vaccine candidates or medically supervised, low-dose oral live virus challenges in low-risk people.
In conclusion, and as argued previously, vaccine protection against infection and “mild disease” has pretty much collapsed, whereas protection against severe disease and death remains at a reasonable level, with the partial exception of the most senior citizens and especially nursing home residents, some of whom have never mounted a neutralizing antibody response to the vaccine. Moreover, future coronavirus variants will likely achieve additional immune evasion.
Reduced BNT162b2 mRNA vaccine response in SARS-CoV-2-naive nursing home residents
Abstract
The SARS-CoV-2 pandemic impact on nursing home (NH) residents prompted their prioritization for early vaccination.
To fill the data gap for vaccine immunogenicity in NH residents, we examined antibody levels after BNT162b2 mRNA vaccine to spike, receptor binding domain (RBD) and for virus neutralization in 149 NH residents and 111 health care worker controls. SARS-CoV-2-naive
NH residents mount antibody responses with nearly 4-fold lower median neutralization titers and half the anti-spike level compared to SARS-CoV-2-naive healthcare workers.
By contrast, SARS-CoV-2-recovered vaccinated NH residents had neutralization, anti-spike and anti-RBD titers similar to SARS-CoV-2-recovered vaccinated healthcare workers.
NH residents’ blunted antibody responses have important implications regarding the quality and durability of protection afforded by neoantigen vaccines. We urgently need better longitudinal evidence on vaccine effectiveness specific to NH resident populations to inform best practices for NH infection control measures, outbreak prevention and potential indication for a vaccine boost.
https://www.medrxiv.org/content/10.1101/2021.03.19.21253920v1
Dr. Simone Gold – The truth about the CV19 vaccine
Dr Simone Gold, talking about new experimental mRNA vaccine, safte, effectivens and in the beginning a couple of minutes about her experience with HCQ but most of this video is about the.
what are the concerns regarding the effectiveness:
Super shocking is that there’s no proof that this biological agent actually stops the transmission amongst people!!
I mean it’s like it’s like a joke right, it’s like the punchline to a joke “let’s take a vaccine and by the way it doesn’t actually stop transmission “
And by the way this is not disputed, it’s been well documented that they do not known if it stops transmission
Is it like putting people into sort of an asymptomatic carrier, turning positive and becoming the new positives! People taking the vaccine and now they’re testing positive for COVID-19 is kind of funny!
Are they going to test positive forever!? 10s or hundreds of millions running around just kind of positive; what does that mean? Are they going to tell us that the cases have risen!?
Jan Bonte (Hommel) – the Pfizer / BionTech SARS-CoV-2 virus Vaccin
A fantastic piece from Jan Bonte (Dutch Neurologist) detailing the Pfizer vaccin with all it’s unknowns in respect of efficacy, side- and adverse effects.
Too bad; only a few on this planet master the Dutch language… but with the help of online translators
This link directs you to the original blog …select your language of choice with this link to google translate ; this link to Microsoft web translator
Enjoy reading
Will covid-19 vaccines save lives? Current trials aren’t designed to tell us
The world has bet the farm on vaccines as the solution to the pandemic, but the trials are not focused on answering the questions many might assume they are. Peter Doshi reports
As phase III trials of covid-19 vaccines reach their target enrolments, officials have been trying to project calm. The US coronavirus czar Anthony Fauci and the Food and Drug Administration leadership have offered public assurances that established procedures will be followed. Only a “safe and effective” vaccine will be approved, they say, and nine vaccine manufacturers issued a rare joint statement pledging not to prematurely seek regulatory review.
But what will it mean exactly when a vaccine is declared “effective”? To the public this seems fairly obvious. “The primary goal of a covid-19 vaccine is to keep people from getting very sick and dying,” a National Public Radio broadcast said bluntly.
…Yet the current phase III trials are not actually set up to prove either. None of the trials currently under way are designed to detect a reduction in any serious outcome such as hospital admissions, use of intensive care, or deaths. Nor are the vaccines being studied to determine whether they can interrupt transmission of the virus.
https://www.bmj.com/content/371/bmj.m4037
FDA Meeting briefing – Pfizer vaccine details revealed
December 12, 2020
It DOES NOT prevent infection or spread of the disease. Masks & social distancing are still required. Of the 3410 individuals who got infected during the study, almost half were from the vaccinated group. The vaccine did not prevent infection!
Page 48
Vaccine effectiveness against transmission of SARS-CoV-2
Data are limited to assess the effect of the vaccine against transmission of SARS-CoV-2 from individuals who are infected despite vaccination.
Demonstrated high efficacy against symptomatic COVID-19 may translate to overall prevention of transmission in populations with high enough vaccine uptake, though it is possible that if efficacy against asymptomatic infection were lower than efficacy against symptomatic infection, asymptomatic cases in combination with reduced mask-wearing and social distancing could result in significant continued transmission.
Additional evaluations including data from clinical trials and from vaccine use post-authorization will be needed to assess the effect of the vaccine in preventing virus shedding and transmission, in particular in individuals with asymptomatic infection.
Online Cook book: https://www.fda.gov/media/144245/download?fbclid=IwAR3ujXu-00dEz9Ro_4LnXTWG5Kt2DCoK1SMoZhpcRiNjWqoKrub1xAGGEM4
MHRA Public Assessment Report BNT162b2 RNA
MHRA Medicines & Healthcare products Regulatory Agency
Public Assessment Report online Authorisation for Temporary Supply
COVID-19 mRNA Vaccine BNT162b2 (BNT162b2 RNA)
concentrate for solution for injection
Department of Health and Social Care (DHSC)
Pfizer Limited & BioNTech Manufacturing GmbH
The full report online
Section “Serious adverse events“
Two deaths were reported in participants that received BNT162b2 in Phase 2/3 of study
c4591001; narratives were provided. A participant died 3 days after Dose 1; the provisional
cause of death was atherosclerotic disease. A participant experienced cardiac arrest 60 days after Dose 2 and died 3 days later.
Vaccination card / passport for EU citizens
Covid-19 vaccines: ethical, legal and practical considerations
https://pace.coe.int/en/files/29004/html
7.3.1 ensure that citizens are informed that the vaccination is NOT mandatory and that no one is politically, socially, or otherwise pressured to get themselves vaccinated, if they do not wish to do so themselves

Children’s Health Defence
https://childrenshealthdefense.org
The Defender is experiencing censorship on many social channels.
Do Vaccines Make Us Healthier?
Three groundbreaking studies examined what federal health officials admit they’ve never investigated — whether vaccines improve overall health. The results were “jaw-dropping.”
Everyone, no matter where they stand on the vaccine debate, should want to know the answer to that question.
In the video you’ll learn about three groundbreaking studies that set out to answer this most basic question.
The 3 studies (below) were conducted independently, using different methods — but all three compared the overall health of vaccinated people versus the overall health of the tiny fraction of people in the U.S. who have never been vaccinated.
https://journals.sagepub.com/doi/10.1177/2050312120925344
https://www.mdpi.com/1660-4601/17/22/8674
https://archive.is/PwUrN
New Analysis: Pfizer Vaccine Killed ‘About 40 Times More Elderly Than the Disease Itself Would Have Killed’
A re-analysis of data from the Israeli Health Ministry concluded Pfizer’s COVID vaccine killed “about 40 times more (elderly) people than the disease itself would have killed” during a recent five-week vaccination period, and 260 times more younger people than would have died from the virus.
While in January a group of independent doctors concluded that experimental COVID-19 vaccines are “not safer” than the virus itself, a new analysis of vaccine-related death rates in Israel demonstrates that this may indeed be the case to dramatic levels.
https://childrenshealthdefense.org/defender/israel-pfizer-vaccine-killed-more-elderly-than-covid/
We Need More Details and the Raw Data
Jan 5, 2021
Peter Doshi: Pfizer and Moderna’s ‘95% Effective’ Vaccines — We Need More Details and the Raw Data
Peter Doshi outlines new concerns about the trustworthiness and meaningfulness of the reported efficacy results of Pfizer’s and Moderna’s COVID-19 vaccine trials.
Flu Vaccine Facts
A compiled list of resources to help you make informed decisions about the flu vaccine in order to protect you and your family from harm.
For instance, mercury (thimerosal) is a neurotoxin and contained in some flu vaccines. It has been linked to neurodevelopmental disorders and many diseases.
CHD Responds to News of Life-Threatening Reaction to Pfizer COVID Vaccine
Polyethylene glycol (PEG) in COVID mRNA vaccines, could cause severe allergic reactions.
CHD’s concerns about PEG stem from the fact that PEG-specific immune responses can actually reduce the efficacy of vaccines and increase the occurrence of adverse events.
RFK, Jr. Warned FDA Three Months Ago About Ingredient in Pfizer COVID Vaccine
Moderna, Pfizer/BioNTech and Arcturus Therapeutics COVID vaccines all utilize a never-before-approved messenger RNA (mRNA) technology, an experimental approach designed to turn the body’s cells into viral protein-making factories. This technology involves the use of lipid nanoparticles (LNPs) that encapsulate the mRNA to protect them from degradation and promote cellular uptake.
The LNP formulations in the three COVID-19 mRNA vaccines are “PEGylated,” meaning that the vaccine nanoparticles are coated with a synthetic, non-degradable and increasingly controversial PEG.
RFK, Jr. Urges FDA to Slow Down COVID Vaccine Approval Process
CHD Asks Journal to Retract Study Saying Flu Vaccines Protect Against COVID
The letter details gross errors in “Considering Interim Interventions to Control COVID-19 Associated Morbidity and Mortality — Perspectives,” an original research paper by Mark Christopher Arokiaraj, published Sept. 22 in Frontiers in Public Health.
After reviewing the paper, Kennedy and Hooker concluded that “because of the nature of the error and the faulty conclusions made from the erroneous results, this paper should be retracted as soon as possible.”
COVID Vaccine Hesitancy Widespread, Even Among Medical Professionals
Seventy-six percent of the vaccine-hesitant healthcare workers cited the “fast-tracked vaccine development” as a primary reason for their concerns. Typically, vaccines take between eight to 10 years to develop, Dr. Emily Erbelding, an infectious disease expert at National Institute of Allergy and Infectious Diseases, told CNN in an article titled, “The timetable for a coronavirus vaccine is 18 months. Experts say that’s risky.”
GSK Recycles Its Problematic Adjuvant into Covid-19 Vaccines
GSK and Sanofi Covid-19 vaccine joint effort.
Under this “unprecedented” arrangement, Sanofi will provide the coronavirus antigen while GSK ponies up its trademark AS03 adjuvant system.
Describing AS03’s mechanisms of action in vaccines, GSK researchers have noted that the adjuvant can induce “rapid perturbation” that activates a response called endoplasmic reticulum (ER) stress. An activated ER stress response has been associated with numerous chronic diseases, and severe ER stress also “threatens proper organ function.” Investigators have described an urgent need to study “the consequences of pharmacological interference with ER stress responses.”
AS03 played out quite differently in Europe, where it featured prominently in GSK’s Pandemrix H1N1 “swine flu” vaccine—widely administered in 2009-2010. The U.S. never licensed Pandemrix. In 2010, after Pandemrix received fast-tracked approval from the European Medicines Agency (EMA) under special rules for declared pandemics, an unusually high number of young people—an estimated 1300 in all—developed severe narcolepsy, “all but wreck[ing] normal life.”
Pentagon Study: Flu Shot Raises Risk of Coronavirus by 36%
On March 12th, 2020, Anderson Cooper and Dr. Sanjay Gupta held a global town hall on “Corona Facts and Fears.” During the discussion, Anderson said to the viewing audience, “And, again, if you are concerned about coronavirus, and you haven’t gotten a flu shot…you should get a flu shot.”
Setting safety and efficacy of influenza vaccination aside, is Anderson’s claim that the flu shot will help people fight COVID-19 remotely true? The short answer is no.
In fact, the results of many peer-reviewed, published studies prove that Anderson’s recommendation may have been the worst advice he could have given the public.
All of the above CHD articles in 1 PDF Binder
SARS-CoV-2 vaccines in development
No vaccines against coronaviruses have yet been licensed for use in humans.

Traditional vaccine development is a lengthy process, and a development time of 15 years is common (Fig. above). The process begins with exploratory work on vaccine design and evaluation in animal models, which can take years.
This is then followed by a stage in which more formal preclinical experiments are conducted, a process for vaccine production is designed and formal toxicology studies are performed; this stage can also last for several years.
Next, an application for an investigational new drug is filed and phase I clinical trials (testing in fewer than 100 individuals; approximately 2 years) are performed to generate an initial safety profile of the vaccine candidate and to obtain preliminary immunogenicity data.
If the results are promising and funding is available, a vaccine candidate is then moved into phase II clinical trials (testing in a few hundred individuals, also lasting about 2 years) to further investigate immunogenicity and to determine an appropriate dose and optimal vaccine regimens.
If the results of phase II trials are encouraging, the decision might be made to move forward with very costly phase III clinical trials (in thousands of individuals; approximately 2 years) in which efficacy and safety are evaluated.
If the outcome of phase III trials meets the pre-defined end points, a biologics license application is filed with regulatory agencies (for example, the United States Food and Drug Administration (FDA) or the European Medicines Agency).
The licensing process can take another 1–2 years, especially if additional data are requested. Importantly, because it is very expensive, the overall process of vaccine development is slowed by economic risk assessment at every step. Vaccine development progresses through these stages only if the developer is convinced that the data are promising, that the risk of failure is relatively low and that there is (still) a market for the vaccine.
– Text below copied from tweet Jan Bonte, Dutch neurologist –
Although vaccine development is moving forward at an unparalleled speed, there are still many open questions. It is likely that two doses of a vaccine will be required, with booster doses potentially necessary at later time points;
in this case, at least 16 billion doses will be needed to meet the global demand. Many of the vaccines that are described below are being developed by entities that have never brought a vaccine to market, or use technologies that have never resulted in a licensed vaccine.
The upper respiratory tract is thought to be mainly protected by secretory IgA, whereas the lower respiratory tract is thought to be mainly protected by IgG. Vaccines that are administered intramuscularly or intradermally induce mainly IgG, and no secretory IgA.
It is therefore possible that most vaccines currently in development induce disease-preventing or disease-attenuating immunity, but not necessarily sterilising immunity.
For SARS-CoV-2 vaccine candidates, there have so far been no signals of enhanced disease in animal models or in humans; however, such a safety signal would certainly derail the development of a vaccine candidate and would negatively affect vaccine development in general.
– Text above copied from tweet. Jan Bonte, Dutch neurologist –
https://www.nature.com/articles/s41586-020-2798-3#citeas
Cytokine Storm
A not to difficult read that gives you a good basic understanding about a “cytokine storm” . In short, cytokine storm involves an immune response that causes collateral damage, which may be greater than the immediate benefit of the immune response.
In short, cytokine storm involves an immune response that causes collateral damage, which may be greater than the immediate benefit of the immune response.
This year marks 10 years since the first description of a cytokine storm that developed after chimeric antigen receptor (CAR) T-cell therapy1 and 27 years since the term was first used in the literature to describe the engraftment syndrome of acute graft- versus-host disease after allogeneic hematopoietic stem-cell transplantation.2 The term “cytokine release syndrome” was coined to describe a similar syndrome after infusion of muromonab-CD3 (OKT3).3 Cytokine storm and cytokine release syn- drome are life-threatening systemic inflammatory syndromes involving elevated levels of circulating cytokines and immune-cell hyperactivation that can be triggered by various therapies, pathogens, cancers, autoimmune conditions, and monogenic disorders.  Covid-19 –Associated Cytokine Storm (starting at page 14) .. characterized by heterogeneous symptoms ranging from mild fatigue to life-threatening pneumonia, cytokine storm, and multiorgan failure.
Covid-19 –Associated Cytokine Storm (starting at page 14) .. characterized by heterogeneous symptoms ranging from mild fatigue to life-threatening pneumonia, cytokine storm, and multiorgan failure.
Cytokine storm was also reported in patients with SARS and was associated with poor out comes.
https://www.nejm.org/doi/pdf/10.1056/NEJMra2026131?articleTools=true
Epigenetics
WHO vaccination policies will increase diseases in all populations
Judy Wilyman PhD The WHO recommendations for vaccines are a one-size fits all and this fact means that these policies will increase diseases in all populations. They cannot be described as ‘protective health policies’ because they contradict the science of epigenetics; the science showing that individuals are pre-disposed to diseases due to their genetic make-up and the interaction with chemicals in the vaccines.
Videos to Watch Regarding the False Media Presentation of COVID19
May 25, 2020 By Judy Wilyman PhD
More information on Vaccinationsdecisions.net
Dr Bruce Lipton – Stress, Epigenetics and more
Stress is a Chemical, it causes the blood vessels to shut down.
Dr Bruce Lipton
If you understand Epigenetic’s you don’t need the Pharmaceutical Industry.
For those who really want to look beyond the current paradigm of Allopathic medicine / allopathy.
The full interview at LondonReal
Dr Bruce Lipton https://www.brucelipton.com
B.A. in biology from C.W. Post Campus of Long Island University in 1966.
PhD in developmental biology from the University of Virginia in 1971.
1973 to 1982 Taught anatomy at the University of Wisconsin School of Medicine, before joining St. George’s University School of Medicine as a professor of anatomy for three years
Epigenetics fundamentals
Epigenetics is the study of heritable changes in gene expression (active versus inactive genes) that do not involve changes to the underlying DNA sequence — a change in phenotype without a change in genotype — which in turn affects how cells read the genes. Epigenetic change is a regular and natural occurrence but can also be influenced by several factors including age, the environment/lifestyle, and disease state. Epigenetic modifications can manifest as commonly as the manner in which cells terminally differentiate to end up as skin cells, liver cells, brain cells, etc. Or, epigenetic change can have more damaging effects that can result in diseases like cancer. At least three systems including DNA methylation, histone modification and non-coding RNA (ncRNA)-associated gene silencing are currently considered to initiate and sustain epigenetic change.1 New and ongoing research is continuously uncovering the role of epigenetics in a variety of human disorders and fatal diseases. Epigenetics Fundamentals
Epigenetics explained in simple terms (3 minutes)
Dr. Eric Berg, DC
Young doctor explains why he’s against forced COVID-19 vaccine
A COVID-19 vaccine should not be mandatory, and getting people to take it “serves certain special interests,” a young medical doctor told LifeSiteNews.
“I have no doubt about it,” Dr. Leland Stillman said when LifeSite’s video reporter Jim Hale asked him if the push for the vaccine had, in many ways, to do with money. Hale spoke with Stillman at the “March Against Mandates” in Richmond, Virginia, last week.
National Childhood Vaccine Injury Act of 1986 – The Legislation that Changed Everything

eBook Conflicts of Interest Undermine Children’s Health
SAGE conflicts of interest
WHO Strategic Advisory Group of Experts (SAGE)
November 9, 2020
Executive summary
* As late as March 11th, 2020, the UK government and medical officers issued practical and minimally disruptive advice to combat the spread of the novel coronavirus.
* On March 16th, the now infamous Neil Ferguson/Imperial College paper was published predicting over 500,000 deaths in the UK and 2.2 million in the US if suppression measures were not introduced.
* Stricter measures were announced on the day that paper was published, and the first UK lockdown was announced a week later, on March 23rd. US states variously followed suit.
* The committee that has been advising the government throughout this period is called the Scientific Advisory Group for Emergencies (SAGE). Ferguson was a member of this committee until he resigned in May for having broken lockdown rules.
* This week’s note examines the key influencers on SAGE and their conflicts of interest:
– Organisations invested in vaccines make money from vaccines. People who acquire natural immunity have less/no need for a vaccine. If people are locked in their homes, they have less chance of acquiring natural immunity.
– Twelve out of 20 key influencers work for/have received funding from organisations involved in the Covid-19 vaccine.
– There are four times more modellers/statisticians and experts in behaviour manipulation on the committee than there are virologists. There are no immunologists.
* It doesn’t matter if a drug is good or bad. It matters that those who have a financial interest in that drug are conflicted if they give advice that protects the financial interest in that drug.
Online https://www.zoeharcombe.com/2020/11/sage-conflicts-of-interest/
MD Stanley Plotkin speaks under oath about vaccine ingredients.
Dr. Stanley Plotkin considered one of the leading experts on vaccines and vaccinations.
In the 1960s, he played a critical role in the development of the rubella vaccine and several manufacturers ask him for his advice.
More videos on this youtube channel
And if you have 9 hours to spare the full version:
Aborted fetal tissues are used in vaccines. Vaccines have been experimentally tested on orphans and on mental handicapped children. Experimental tests on babies from mothers in prisons. Experimental tests on 1 million people in then colonial Belgian Congo. Shocking video.
Dr. Carrie Madej – My alarm call to the world
Internal Medicine Specialist in McDonough, GA Graduated from Kansas City Univ Of Medicine Bioscience College Of Osteopathic Medicine medical school in 2001. Affiliated with medical facilities Piedmont Fayette Hospital and Southern Regional Medical Center.
RNA vaccines, classes of vaccine that has never been approved for human use in the U.S. and involve injecting foreign genetic material into the human body. Notably, it is this very class of vaccine, now being produced by DARPA-partnered companies, that billionaire and global health “philanthropist” Bill Gates recently asserted has him “most excited” relative to other Covid-19 vaccine candidates. Yet, key aspects regarding these vaccines and other DARPA “healthcare” initiatives have been left out of these recent positive reports.
Watch this highly informative video by physician Dr. Carrie Madej, explaining the 3 major components of the Moderna vaccine and the implications.
If we allow the mandatory vaccination rhetoric to proceed , humans will no longer be human. Dr. Madej does an outstanding job going into greater detail. Remember, the function of RNA is to repair and re-write the DNA.
Another great article on this subject:
FDA Nears Approval of Injectable Biochip Implants for COVID Detection
The Department of Defense, and the Bill and Melinda Gates Foundation, have partnered with a Silicon Valley company, Profusa, to implement a technology which could control our minds and bodies. What may seem like science fiction, is in fact happening in real-time.
A permanent chip made of an advanced material called hydrogel irreversibly ties humans to the Internet “cloud.” The chip, about the size of a grain of rice, provides feedback to a database on changes in body chemistry and other biometrics. The company says technology will be used to detect COVID in the general population, before symptoms show.
The latest revised CDC overall survival rate for the COVID virus is 99.8%, versus 99.9% for the common flu. Nevertheless, nearly 150 days after governments proclaimed that 15 days of “lockdowns” and social distancing would be necessary to “flatten the curve” so that hospitals would not be overwhelmed, US governors still exert emergency powers based on the announcement of “new cases.”
Full article: https://steemit.com/covid/@munkle/permanent-injectable-biochip-covid-sensors-near-fda-approval Reader view backup:
Robert F Kennedy Jr. at Londonreal.tv
My fight agains mandatory vaccinations, big pharma and Dr. Fauci
Children’s Health Defense; Measles Vaccination and Autism
In a surprisingly candid systematic review of the autoantibody literature just published in Research in Autism Spectrum Disorders, authors from Harvard and other American universities cite long-standing evidence that viral vaccines—and explicitly the MMR—are one of the culprits capable of knocking the immune system off its game.
Instagram video July 7, 2020 Robert f Kennedy; discussion with Dr. Andy Lakefied
Influenza vaccination and respiratory virus interference
Vaccinated individuals may be at increased risk for other respiratory viruses because they do not receive the non-specific immunity associated with natural infection.
Additionally, the laboratory data in our study showed increased odds of coronavirus and human metapneumovirus in individuals receiving influenza vaccination.
The overall results of the study showed little to no evidence supporting the association of virus interference and influenza vaccination.
https://europepmc.org/article/MED/31607599
Does the Flu Shot Increase COVID-19 Risk (YES!)
Dr. Michael Murray This may be the most important newsletter I have written to date. Here are a few quick answers to the questions I will cover in case you aren’t interested in the whole story:
- Does the flu shot increase the risk for coronavirus infection? YES!
- Could a new flu vaccine be partly responsible for the COVID-19 mortality rate in Italy? YES!
- Is the rush to a vaccine the best solution? No, it could bring catastrophic results.
- How does the SARS-CoV-2 infect and are protease enzyme supplements the key to creating our own endogenous antiviral protease inhibitors? Yes, I believe so!
- Are there certain medications like blood pressure drugs and proton pump inhibitors that increase risk for infection and mortality? YES
- Is it chloroquine or is it zinc that is working as a possible aid in treating COVID-19? A strong case can be made for zinc!
- Can plant polyphenols and flavonoids act to increase the antiviral effects of zinc? YES! And they possess other benefits too!
Flu shots contain suspect ingredients, carcinogen formaldehyde, mercury in the form of thimerosal.
“Mercury is one of the most poisonous substances known to mankind,” Dr. Brownstein tells Newsmax Health. “It is a potent neurotoxin and is associated with a host of neurological and immune system problems. Mercury should never be injected into any living human being.”
Thimerosal, a preservative found in many flu shots, is 50 percent mercury. It’s different, and much more harmful, than the type of mercury found in fish. While the FDA warns against eating more than two servings of fish weekly because of the danger of mercury, it allows this more toxic form to be added to flu shots (and other vaccines).
“There’s no doubt that the flu vaccine can lead to Alzheimer’s, because many flu shots are preserved with mercury and it’s a known brain toxin,” says Dr. Brownstein. “You give enough brain toxins and people are going to develop memory issues.”
“Those promoting flu shots promise they’ll cut your risk of getting flu by more than 50 percent, but that’s simply not true. When you dissect the studies, you’ll find the FluLaval vaccine is 97 percent ineffective.”
Full article https://www.newsmax.com/Health/Headline/flu-shots-vaccine-thimerosal/2014/11/20/id/608614/
An aluminium adjuvant in a vaccine is an acute exposure to aluminium
Simply by looking at just one dose of a vaccine given at 8 weeks of age it is abundantly clear that science does not support this contention, as espoused regularly by many infant paediatricians. In fact, just a single dose of Infanrix Hexa vaccine represents a severe acute exposure to systemically available aluminium.
A single dose of this vaccine is equivalent to the exposure to aluminium that an infant would receive from 150 days breast-feeding. It is equivalent to 25 times the daily dose of aluminium received from the most contaminated of infant formulas. It is pertinent to emphasise that an infant would receive a further two doses of this vaccine during the aforementioned 150 day period. It is also highly relevant that other aluminium adjuvanted vaccines, for example Prevenar 13 (https://www.medicines.org.uk/emc/product/453/smpc) and Men B (https://www.medicines.org.uk/emc/product/5168/smpc) are also part of the infant vaccine schedule for this same period.
In the United Kingdom it is not uncommon for an infant to receive all three of these aluminium adjuvanted vaccines on the same day. A combined daily exposure of 1.445 mg of aluminium (according to the manufacturer’s data), equivalent to 260 days exposure to aluminium through breast feeding. Exposure to aluminium through a vaccine is, in comparison to diet, an acute exposure and an infant’s physiology will respond differently to exposure to a high concentration of aluminium over a very short time period. The latter, acute versus chronic exposure, while not yet being taken into account in infant vaccination programmes, must now be considered to help to ensure that future vaccination schedules are safe. Currently the EMA and the FDA limit the aluminium content of a vaccine to 1.25 mg (See for example, https://www.ecfr.gov/cgi-bin/text-idx?SID=832c22988b6c802fe810e16ea34ace1a&mc=true&node=se21.7.610_115&rgn=div8). This limit is based upon the aluminium adjuvant’s efficacy in inducing antibody titres.
Perhaps now is the time to revise this limit based upon additional factors of vaccine safety.
https://www.sciencedirect.com/science/article/pii/S0946672X19304201?via%3Dihub
Past vaccine disasters show why rushing would be ‘colossally stupid’
CNN Health’s Jamie Gumbrecht contributed to this story
Vaccine experts are warning the federal government against rushing out a coronavirus vaccine before testing has shown it’s both safe and effective. Decades of history show why they’re right.
https://edition.cnn.com/2020/09/01/health/eua-coronavirus-vaccine-history/index.html Reader view backup for download:
Mandatory Vaccination consider this
Stop the Covid Holocaust! Open Letter
Ladies and Gentlemen,
We, the survivors of the atrocities committed against humanity during the Second World War, feel bound to follow our conscience and write this letter.
It is obvious to us that another holocaust of greater magnitude is taking place before our eyes. The majority of the world’s populace do not yet realize what is happening, for magnitude of an organized crime such as this is beyond their scope of experience.
We, however, know. We remember the name Josef Mengele. Some of us have personal memories. We experience a déjà vu that is so horrifying that we rise to shield our poor fellow humans.
The threatened innocents now include children, and even infants. In just four months, the COVID-19 vaccines have killed more people than all available vaccines combined from mid-1997 until the end of 2013—a period of 15.5 years. And people affected worst are between 18 and 64 years old – the group which was not in the Covid statistics.
We call upon you to stop this ungodly medical experiment on humankind immediately. What you call “vaccination” against SARS-Cov-2 is in truth a blasphemic encroachment into nature. Never before has immunization of the entire planet been accomplished by delivering a synthetic mRNA into the human body.
It is a medical experiment to which the Nuremberg Code must be applied. The 10 ethical principles in this document represents a foundational code of medical ethics that was formulated during the Nuremberg Doctors Trial to ensure that human beings will never again be subjected to involuntary medical experimentation & procedures.
https://www.globalresearch.ca/stop-the-covid-holocaust-open-letter
The issues raised by the Nuremberg trials are as relevant to medicine in 1996 (and 2020) as in 1946
The Nuremberg trials of doctors who had committed war crimes during the second world war began 50 years ago this week.
The BMJ has devoted many pages in this issue to exploring the Nuremberg trials, what went before, and their aftermath for two main reasons.
Firstly, we must never forget. On the wall of the highly moving United States Holocaust Museum is a quote from Deuteronomy: “Only guard yourself and your soul carefully, lest you forget the things your eyes saw.”
Secondly, the issues thrown up by the trials–informed consent for experimentation, the involvement of doctors with the state, patient autonomy, genocide, and the behaviour of doctors when associated with abuses of human rights–are as relevant today as the day the trials began.
Indeed, there is a sense, particularly in Germany, that we are at the very beginning of thinking through the issues thrown up by what doctors did in the second world war.
We needed 50 years to be able to begin to think clearly about something so horrible.
– the whole story via this link or download pdf backup below.
Universal Declaration on Bioethics and Human Rights
1. Any preventive, diagnostic and therapeutic medical intervention is only to be carried out with the prior, free and informed consent of the person concerned, based on adequate information. The consent should, where appropriate, be express and may be withdrawn by the person concerned at any time and for any reason without disadvantage or prejudice.
2. Scientific research should only be carried out with the prior, free, express and informed consent of the person concerned. The information should be adequate, provided in a comprehensible form and should include modalities for withdrawal of consent. Consent may be withdrawn by the person concerned at any time and for any reason without any disadvantage or prejudice. Exceptions to this principle should be made only in accordance with ethical and legal standards adopted by States, consistent with the principles and provisions set out in this Declaration, in particular in Article 27, and international human rights law.
3. In appropriate cases of research carried out on a group of persons or a community, additional agreement of the legal representatives of the group or community concerned may be sought. In no case should a collective community agreement or the consent of a community leader or other authority substitute for an individual’s informed consent.
The ten points of the Nuremberg Code
- Voluntary consent is essential
- The results of any experiment must be for the greater good of society
- Human experiments should be based on previous animal experimentation
- Experiments should be conducted by avoiding physical/mental suffering and injury
- No experiments should be conducted if it is believed to cause death/disability
- The risks should never exceed the benefits
- Adequate facilities should be used to protect subjects
- Experiments should be conducted only by qualified scientists
- Subjects should be able to end their participation at any time
- The scientist in charge must be prepared to terminate the experiment when injury, disability, or death is likely to occur
http://www.cirp.org/library/ethics/nuremberg/
https://www.bmj.com/content/313/7070/1448.1.full
Declaration of Helsinki
ETHICAL PRINCIPLES FOR MEDICAL RESEARCH INVOLVING HUMAN SUBJECTS.
The World Medical Association (WMA) has developed the Declaration of Helsinki as a statement of ethical principles for medical research involving human subjects, including research on identifiable human material and data.
Council of Europe
Convention for the protection of Human Rights and Dignity of the Human Being with regard to the Application of Biology and Medicine: Convention on Human Rights and Biomedicine: https://www.coe.int/en/web/conventions/full-list/-/conventions/treaty/164
Chapter II – Consent
Article 5 – General rule
An intervention in the health field may only be carried out after the person concerned has given free and informed consent to it.
This person shall beforehand be given appropriate information as to the purpose and nature of the intervention as well as on its consequences and risks.
The person concerned may freely withdraw consent at any time.
This Declaration addresses ethical issues related to medicine, life sciences and associated technologies as applied to human beings.
NIH National Library of Medicine
Abstract
The Convention on Human Rights and Biomedicine developed by the Council of Europe, now undergoing ratification, is the first international treaty focused on bioethics. This article describes the background of the Convention’s development and its general provisions and provides a comparison of its requirements with those of federal regulations governing research with human subjects. Although most provisions are comparable, there are significant differences in scope and applicability, for example, in the areas of compensation for injury, research participation by persons with limited capacity to consent, assisted reproduction, organ transplantation, and research in emergency situations. The Convention represents a milestone in international bioethics and protection of human rights that will probably be referred to with increasing frequency
http://portal.unesco.org/en/ev.php-URL_ID=31058&URL_DO=DO_PRINTPAGE&URL_SECTION=201.html
United Nations Educational, Scientific and Cultural Organization
The Convention on Human Rights and Biomedicine of the Council of Europe
A parent doctor discussion on Immunization / Vaccination
Doctor: Is your child immunized?
Me: Yes
Doctor: It’s not in his records.
Me: Why would it be?
Doctor: What do you mean?
Me: What do you mean?
Doctor: Who immunized your child?
Me: My wife and I.
Doctor: What do you mean?
Me: What do you mean?
Doctor: How did you and your wife immunize your child?
Me: She birthed him naturally at home and breastfed him for the first year and a half of his life, and we both make sure he eats nutritionally dense organic foods. We also make sure he spends a lot of time in the sun moving his body daily out in nature connected to the earth, and pretty much only drinks water that comes straight from a natural spring without any fluoride or chlorine in it.
Doctor: But I asked you if your child has been vaccinated, and you said “yes!”
Me: No, you asked me if my child has been immunized, and I said “yes.”
Doctor: Vaccinations…immunizations…same thing!
Me: Uhhh…you keep using that word, but I don’t think you know what it means…
Doctor: What do you mean?
Me: What do you mean?
Doctor: (visibly frustrated) Never mind. Are you going to have him vaccinated or not?
Me: Why would I?
Doctor: So he doesn’t get sick.
Me: But he doesn’t get sick now.
Doctor: Never?
Me: Not really, ….
The Biderman Report of 1956 and Covid-19
‘The truth, when you finally chase it down is almost always far worse than your darkest visions and fears.’
— Hunter S. Thompson
In 1956, there was a study of the impacts of trauma-based mind control on Korean War prisoners detained by communists in North Korea and China. It was call the Biderman Report. Another document followed in 1961. What follows are observations from those documents.
The fear of being controlled by others, with the consequent loss of the autonomy, is believed to be fundamental to the conception of the self and the will.
Communist Coercive methods for eliciting individual compliance

Biderman’s Chart of Coercion
A tool designed to demonstrate and explain the coercive methods of stress manipulation used to torture prisoners of war. It has been applied to explain the coercive techniques used by perpetrators of domestic abuse.
This list directly reflects the original chart, it has not been changed to fit the domestic abuse context. Biderman Report
DNA vs. RNA – 5 Key Differences and Comparison
Deoxyribonucleic acid (DNA) and Ribonucleic acid (RNA) are perhaps the most important molecules in cell biology, responsible for the storage and reading of genetic information that underpins all life. They are both linear polymers, consisting of sugars, phosphates and bases, but there are some key differences which separate the two.
I have never been critical against any vaccine whatsoever; have had all my vaccinations in the 60’s, some more serving the Dutch navy (1978) and in 2010 another 3 shots due to business travel.
Rushing a vaccine with a technology never registered anywhere in the world before; for a virus with a global iFR 0.15-0.20% (0.03-0.04% in those <70 years) [source John P. A. Ioannidis] to me is utterly madness.
Anyone with a healthy brain should think beyond general statements broadcasted by the main stream media, be critical, questioning the information and do his/her own research.
BOOK: VACCINATION proved Useless & Dangerous.
VACCINATION proved Useless & Dangerous from 45yrs of registration statistics by Alfred R. Wallace, 1889
https://archive.org/details/b2136140x/mode/2up?view=theater

COVID19 is a Pandemic of fear, fleeing in logic in which we restrict reality, resulting in destroying society and at the same time creating dangerous social mechanisms.